Emma Rademaker, Daan F L Filippini, Jelle L G Haitsma Mulier, Marleen A Slim, Rombout B E van Amstel, Sivasubramanium V Bhavani, Nicole P Juffermans, Harm-Jan S de Grooth, Lennie P G Derde, Olaf L Cremer, Lieuwe D J Bos
{"title":"托珠单抗对COVID-19急性呼吸窘迫综合征呼吸亚表型的免疫生物学影响","authors":"Emma Rademaker, Daan F L Filippini, Jelle L G Haitsma Mulier, Marleen A Slim, Rombout B E van Amstel, Sivasubramanium V Bhavani, Nicole P Juffermans, Harm-Jan S de Grooth, Lennie P G Derde, Olaf L Cremer, Lieuwe D J Bos","doi":"10.1186/s40635-025-00779-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Two distinct longitudinal respiratory subphenotypes have recently been described in COVID-19-related acute respiratory distress syndrome (ARDS). These subphenotypes exhibit dynamic immunobiological changes that may help guide immunomodulatory interventions. However, the extent to which the immune response is determined by respiratory subphenotype in the presence of concurrent immunomodulatory treatment remains unclear. We investigated the independent and combined effects of respiratory subphenotype and tocilizumab on inflammatory response and clinical outcomes.</p><p><strong>Methods: </strong>We analyzed patients from existing COVID-19 biobanks who were consecutively admitted to the ICU and received more than 4 days of invasive mechanical ventilation between March 2020 and May 2022. Patients were classified into two previously described longitudinal respiratory subphenotypes-characterized by mechanical power, minute volume and ventilatory ratio-referred to as 'low-power' and 'high-power' subphenotypes. We analyzed how tocilizumab treatment and respiratory subphenotype were associated with endothelial and inflammatory plasma biomarkers on days 0, 4 and 7, as well as with mortality.</p><p><strong>Results: </strong>720 patients were included, of whom 464 (64%) and 256 (36%) were assigned to the low- and high-power subphenotypes, respectively. 108 (23%) of the low-power subphenotype patients received tocilizumab, and 43 (17%) of the high-power subphenotype. 427 patients had plasma samples available. The high-power subphenotype was associated with slightly higher SP-D, thrombomodulin and TNF-RI plasma concentrations on the day of intubation compared to the low-power subphenotype, along with a more rapid increase in IL-6 and TNF-RI levels in subjects who had received tocilizumab treatment (β = 0.14 log ng/ml, p = 0.022, and β = 0.06 log ng/ml, p = 0.014, respectively). Tocilizumab treatment accounted for four times more variance in IL-6 and angiopoietin-2 levels than subphenotype, while subphenotype explained only a small proportion of the variance and slightly more than tocilizumab for TNF-RI and thrombomodulin. Subphenotype did not modify the association between tocilizumab and mortality (IPTW adjusted hazard ratio 1.18; 95%CI 0.60-2.33).</p><p><strong>Conclusion: </strong>Respiratory subphenotypes showed varying TNF-RI and IL-6 responses to tocilizumab, but these differences were only minor compared to the drug's overall immunobiological effect. This suggests that respiratory subphenotype should not determine tocilizumab treatment decisions.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"70"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240919/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immunobiological effects of tocilizumab across respiratory subphenotypes in COVID-19 ARDS.\",\"authors\":\"Emma Rademaker, Daan F L Filippini, Jelle L G Haitsma Mulier, Marleen A Slim, Rombout B E van Amstel, Sivasubramanium V Bhavani, Nicole P Juffermans, Harm-Jan S de Grooth, Lennie P G Derde, Olaf L Cremer, Lieuwe D J Bos\",\"doi\":\"10.1186/s40635-025-00779-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Two distinct longitudinal respiratory subphenotypes have recently been described in COVID-19-related acute respiratory distress syndrome (ARDS). These subphenotypes exhibit dynamic immunobiological changes that may help guide immunomodulatory interventions. However, the extent to which the immune response is determined by respiratory subphenotype in the presence of concurrent immunomodulatory treatment remains unclear. We investigated the independent and combined effects of respiratory subphenotype and tocilizumab on inflammatory response and clinical outcomes.</p><p><strong>Methods: </strong>We analyzed patients from existing COVID-19 biobanks who were consecutively admitted to the ICU and received more than 4 days of invasive mechanical ventilation between March 2020 and May 2022. Patients were classified into two previously described longitudinal respiratory subphenotypes-characterized by mechanical power, minute volume and ventilatory ratio-referred to as 'low-power' and 'high-power' subphenotypes. We analyzed how tocilizumab treatment and respiratory subphenotype were associated with endothelial and inflammatory plasma biomarkers on days 0, 4 and 7, as well as with mortality.</p><p><strong>Results: </strong>720 patients were included, of whom 464 (64%) and 256 (36%) were assigned to the low- and high-power subphenotypes, respectively. 108 (23%) of the low-power subphenotype patients received tocilizumab, and 43 (17%) of the high-power subphenotype. 427 patients had plasma samples available. The high-power subphenotype was associated with slightly higher SP-D, thrombomodulin and TNF-RI plasma concentrations on the day of intubation compared to the low-power subphenotype, along with a more rapid increase in IL-6 and TNF-RI levels in subjects who had received tocilizumab treatment (β = 0.14 log ng/ml, p = 0.022, and β = 0.06 log ng/ml, p = 0.014, respectively). Tocilizumab treatment accounted for four times more variance in IL-6 and angiopoietin-2 levels than subphenotype, while subphenotype explained only a small proportion of the variance and slightly more than tocilizumab for TNF-RI and thrombomodulin. Subphenotype did not modify the association between tocilizumab and mortality (IPTW adjusted hazard ratio 1.18; 95%CI 0.60-2.33).</p><p><strong>Conclusion: </strong>Respiratory subphenotypes showed varying TNF-RI and IL-6 responses to tocilizumab, but these differences were only minor compared to the drug's overall immunobiological effect. This suggests that respiratory subphenotype should not determine tocilizumab treatment decisions.</p>\",\"PeriodicalId\":13750,\"journal\":{\"name\":\"Intensive Care Medicine Experimental\",\"volume\":\"13 1\",\"pages\":\"70\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12240919/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Intensive Care Medicine Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40635-025-00779-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00779-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
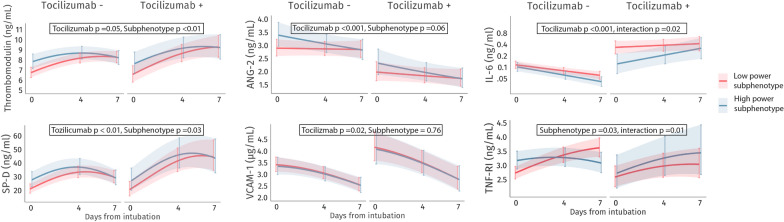
背景:最近在covid -19相关急性呼吸窘迫综合征(ARDS)中描述了两种不同的纵向呼吸亚表型。这些亚表型表现出动态的免疫生物学变化,可能有助于指导免疫调节干预。然而,在同时进行免疫调节治疗的情况下,免疫反应在多大程度上是由呼吸亚表型决定的,目前尚不清楚。我们研究了呼吸亚表型和托珠单抗对炎症反应和临床结果的独立和联合影响。方法:对2020年3月至2022年5月期间连续入住ICU并接受4天以上有创机械通气的现有COVID-19生物库患者进行分析。患者被分为两种先前描述的纵向呼吸亚表型-以机械功率,分气量和通气量比为特征-称为“低功率”和“高功率”亚表型。我们分析了托珠单抗治疗和呼吸亚表型如何与第0、4和7天内皮和炎症血浆生物标志物以及死亡率相关。结果:纳入720例患者,其中464例(64%)和256例(36%)分别被分配到低和高功率亚表型。108例(23%)低功率亚表型患者接受tocilizumab治疗,43例(17%)高功率亚表型患者接受tocilizumab治疗。427名患者有血浆样本。与低功率亚表型相比,高功率亚表型与插管当日稍高的SP-D、血栓调节素和TNF-RI血浆浓度相关,同时接受托珠单抗治疗的受试者IL-6和TNF-RI水平增加更快(β = 0.14 log ng/ml, p = 0.022, β = 0.06 log ng/ml, p = 0.014)。托珠单抗治疗在IL-6和血管生成素-2水平上的差异是亚表型组的四倍,而亚表型组只解释了一小部分差异,而在TNF-RI和血栓调节素方面的差异略高于托珠单抗。亚表型并未改变托珠单抗与死亡率之间的关联(IPTW校正风险比1.18;95%可信区间0.60 - -2.33)。结论:呼吸亚表型对tocilizumab表现出不同的TNF-RI和IL-6反应,但与药物的整体免疫生物学效应相比,这些差异只是次要的。这表明呼吸亚表型不应该决定托珠单抗的治疗决策。
Immunobiological effects of tocilizumab across respiratory subphenotypes in COVID-19 ARDS.
Background: Two distinct longitudinal respiratory subphenotypes have recently been described in COVID-19-related acute respiratory distress syndrome (ARDS). These subphenotypes exhibit dynamic immunobiological changes that may help guide immunomodulatory interventions. However, the extent to which the immune response is determined by respiratory subphenotype in the presence of concurrent immunomodulatory treatment remains unclear. We investigated the independent and combined effects of respiratory subphenotype and tocilizumab on inflammatory response and clinical outcomes.
Methods: We analyzed patients from existing COVID-19 biobanks who were consecutively admitted to the ICU and received more than 4 days of invasive mechanical ventilation between March 2020 and May 2022. Patients were classified into two previously described longitudinal respiratory subphenotypes-characterized by mechanical power, minute volume and ventilatory ratio-referred to as 'low-power' and 'high-power' subphenotypes. We analyzed how tocilizumab treatment and respiratory subphenotype were associated with endothelial and inflammatory plasma biomarkers on days 0, 4 and 7, as well as with mortality.
Results: 720 patients were included, of whom 464 (64%) and 256 (36%) were assigned to the low- and high-power subphenotypes, respectively. 108 (23%) of the low-power subphenotype patients received tocilizumab, and 43 (17%) of the high-power subphenotype. 427 patients had plasma samples available. The high-power subphenotype was associated with slightly higher SP-D, thrombomodulin and TNF-RI plasma concentrations on the day of intubation compared to the low-power subphenotype, along with a more rapid increase in IL-6 and TNF-RI levels in subjects who had received tocilizumab treatment (β = 0.14 log ng/ml, p = 0.022, and β = 0.06 log ng/ml, p = 0.014, respectively). Tocilizumab treatment accounted for four times more variance in IL-6 and angiopoietin-2 levels than subphenotype, while subphenotype explained only a small proportion of the variance and slightly more than tocilizumab for TNF-RI and thrombomodulin. Subphenotype did not modify the association between tocilizumab and mortality (IPTW adjusted hazard ratio 1.18; 95%CI 0.60-2.33).
Conclusion: Respiratory subphenotypes showed varying TNF-RI and IL-6 responses to tocilizumab, but these differences were only minor compared to the drug's overall immunobiological effect. This suggests that respiratory subphenotype should not determine tocilizumab treatment decisions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


