{"title":"实性和囊性肾小肿块的鉴别:多期CT标记物在预测恶性组织学、亚型和分级中的作用。","authors":"Yulian Mytsyk","doi":"10.5114/pjr/202588","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to assess the diagnostic performance of multiphase contrast-enhanced computed tomography (MCECT) in differentiating benign and malignant solid and cystic small renal masses (SRMs), predicting histologic subtypes, and grading, using signal intensity (SI) and tumour-to-cortex signal intensity (TCSI) ratio.</p><p><strong>Material and methods: </strong>A retrospective analysis was conducted on 181 patients with solid and cystic SRMs (≤ 4 cm). MCECT imaging across 4 phases (non-contrast, corticomedullary, nephrographic, and excretory) was performed. SI and TCSI values were measured, and their diagnostic performance was evaluated using receiver operating characteristic (ROC) analysis. Solid, Bosniak IIF, III, and IV SRMs underwent histopathological confirmation.</p><p><strong>Results: </strong>Among solid SRMs, excretory phase SI achieved an area under the curve (AUC) of 0.848 for differentiating RCC from other SRMs, with 100% sensitivity and 61.3% specificity. For distinguishing renal cell carcinoma (RCC) from benign SRMs, the most effective parameter was the TCSI ratio obtained from computed tomography excretory phase (88.6% sensitivity, 52.4% specificity, 0.763 AUC). For Bosniak IIF cysts, the corticomedullary phase SI provided an AUC of 0.902, with 93% sensitivity and 87.5% specificity. RCC subtyping showed distinct SI characteristics across phases, particularly for clear cell RCC. Nephrographic phase SI differentiated low- versus high-grade RCC, with an AUC of 0.901, 90.2% sensitivity, and 86.4% specificity.</p><p><strong>Conclusions: </strong>MCECT-derived imaging biomarkers, particularly SI and TCSI, are effective non-invasive tools for characterising SRMs, aiding in the differentiation of benign and malignant lesions, histological subtypes, and tumour grades. Their integration with advanced radiomics could further enhance diagnostic accuracy.</p>","PeriodicalId":94174,"journal":{"name":"Polish journal of radiology","volume":"90 ","pages":"e239-e252"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12232405/pdf/","citationCount":"0","resultStr":"{\"title\":\"Differentiation of solid and cystic small renal masses: the role of multiphase CT markers in predicting malignant histology, subtype, and grade.\",\"authors\":\"Yulian Mytsyk\",\"doi\":\"10.5114/pjr/202588\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study aimed to assess the diagnostic performance of multiphase contrast-enhanced computed tomography (MCECT) in differentiating benign and malignant solid and cystic small renal masses (SRMs), predicting histologic subtypes, and grading, using signal intensity (SI) and tumour-to-cortex signal intensity (TCSI) ratio.</p><p><strong>Material and methods: </strong>A retrospective analysis was conducted on 181 patients with solid and cystic SRMs (≤ 4 cm). MCECT imaging across 4 phases (non-contrast, corticomedullary, nephrographic, and excretory) was performed. SI and TCSI values were measured, and their diagnostic performance was evaluated using receiver operating characteristic (ROC) analysis. Solid, Bosniak IIF, III, and IV SRMs underwent histopathological confirmation.</p><p><strong>Results: </strong>Among solid SRMs, excretory phase SI achieved an area under the curve (AUC) of 0.848 for differentiating RCC from other SRMs, with 100% sensitivity and 61.3% specificity. For distinguishing renal cell carcinoma (RCC) from benign SRMs, the most effective parameter was the TCSI ratio obtained from computed tomography excretory phase (88.6% sensitivity, 52.4% specificity, 0.763 AUC). For Bosniak IIF cysts, the corticomedullary phase SI provided an AUC of 0.902, with 93% sensitivity and 87.5% specificity. RCC subtyping showed distinct SI characteristics across phases, particularly for clear cell RCC. Nephrographic phase SI differentiated low- versus high-grade RCC, with an AUC of 0.901, 90.2% sensitivity, and 86.4% specificity.</p><p><strong>Conclusions: </strong>MCECT-derived imaging biomarkers, particularly SI and TCSI, are effective non-invasive tools for characterising SRMs, aiding in the differentiation of benign and malignant lesions, histological subtypes, and tumour grades. Their integration with advanced radiomics could further enhance diagnostic accuracy.</p>\",\"PeriodicalId\":94174,\"journal\":{\"name\":\"Polish journal of radiology\",\"volume\":\"90 \",\"pages\":\"e239-e252\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12232405/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Polish journal of radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5114/pjr/202588\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Polish journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pjr/202588","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Differentiation of solid and cystic small renal masses: the role of multiphase CT markers in predicting malignant histology, subtype, and grade.
Purpose: This study aimed to assess the diagnostic performance of multiphase contrast-enhanced computed tomography (MCECT) in differentiating benign and malignant solid and cystic small renal masses (SRMs), predicting histologic subtypes, and grading, using signal intensity (SI) and tumour-to-cortex signal intensity (TCSI) ratio.
Material and methods: A retrospective analysis was conducted on 181 patients with solid and cystic SRMs (≤ 4 cm). MCECT imaging across 4 phases (non-contrast, corticomedullary, nephrographic, and excretory) was performed. SI and TCSI values were measured, and their diagnostic performance was evaluated using receiver operating characteristic (ROC) analysis. Solid, Bosniak IIF, III, and IV SRMs underwent histopathological confirmation.
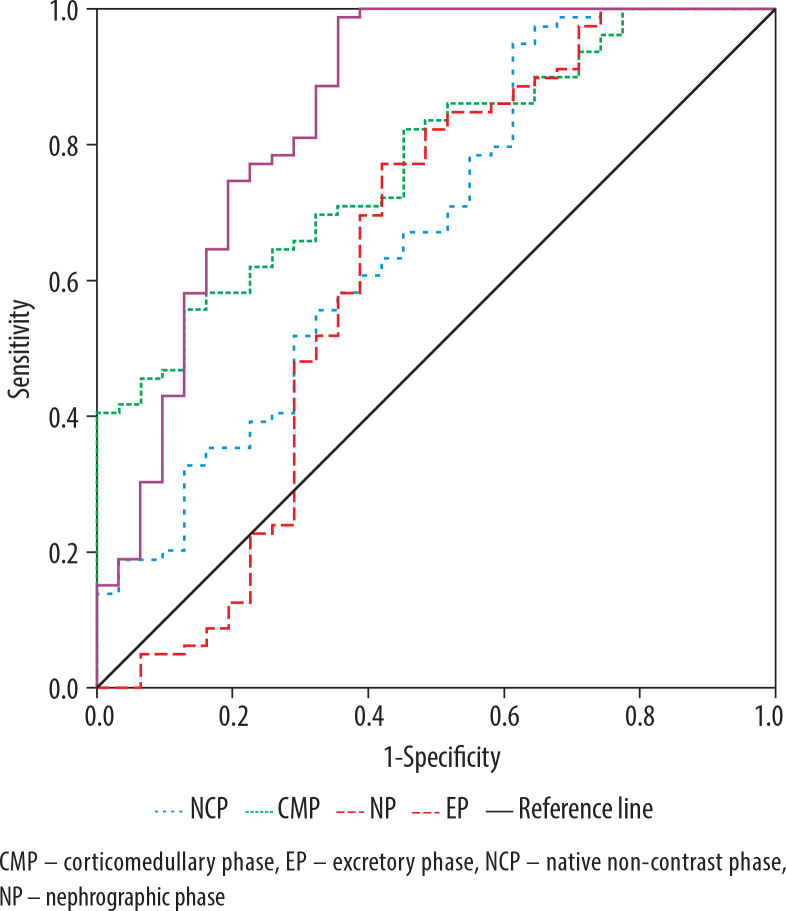
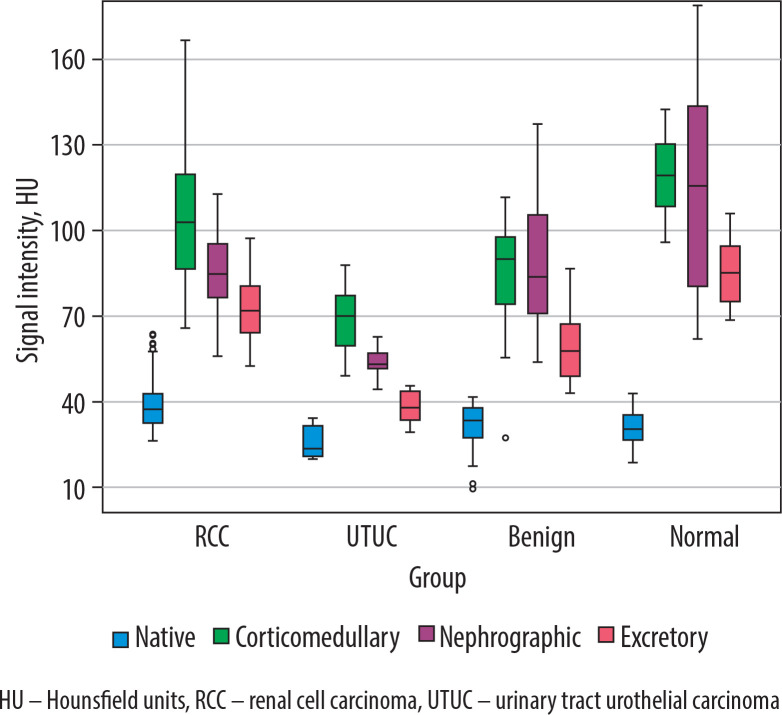
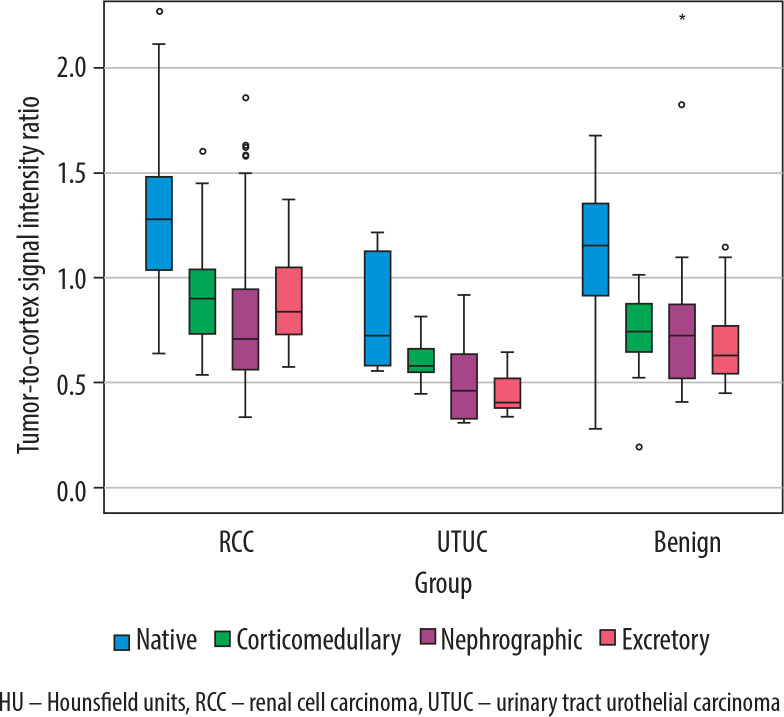
Results: Among solid SRMs, excretory phase SI achieved an area under the curve (AUC) of 0.848 for differentiating RCC from other SRMs, with 100% sensitivity and 61.3% specificity. For distinguishing renal cell carcinoma (RCC) from benign SRMs, the most effective parameter was the TCSI ratio obtained from computed tomography excretory phase (88.6% sensitivity, 52.4% specificity, 0.763 AUC). For Bosniak IIF cysts, the corticomedullary phase SI provided an AUC of 0.902, with 93% sensitivity and 87.5% specificity. RCC subtyping showed distinct SI characteristics across phases, particularly for clear cell RCC. Nephrographic phase SI differentiated low- versus high-grade RCC, with an AUC of 0.901, 90.2% sensitivity, and 86.4% specificity.
Conclusions: MCECT-derived imaging biomarkers, particularly SI and TCSI, are effective non-invasive tools for characterising SRMs, aiding in the differentiation of benign and malignant lesions, histological subtypes, and tumour grades. Their integration with advanced radiomics could further enhance diagnostic accuracy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


