Susan Dent, Heather Moore, Michael Fradley, Chloe Grace Rose, Stella Stergiopoulos, Connie Chen, Benjamin Li, Avirup Guha
{"title":"QT STAR:在一线接受CDK4/6抑制剂的HR+/HER2转移性乳腺癌患者中同时使用延长qtc的药物","authors":"Susan Dent, Heather Moore, Michael Fradley, Chloe Grace Rose, Stella Stergiopoulos, Connie Chen, Benjamin Li, Avirup Guha","doi":"10.1186/s40959-025-00364-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The risk of drug-induced corrected QT interval (QTc) prolongation is an important consideration in clinical decision-making for patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) metastatic breast cancer (mBC). This retrospective analysis described concomitant QTc-prolonging medication use in patients with HR+/HER2- mBC who received first-line (1L) treatment with a cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus an aromatase inhibitor (AI).</p><p><strong>Methods: </strong>This retrospective claims analysis utilized the Optum Clinformatics Data Mart database to identify patients with HR+/HER2- mBC who initiated 1L CDK4/6i plus AI treatment between January 2017 and March 2022. Exposure to QTc-prolonging medications (overall and by Torsades de Pointes [TdP] risk, per www.crediblemeds.org ) was assessed at index (i.e., CDK4/6i treatment initiation) and during follow-up (i.e., duration of CDK4/6i treatment) in the overall cohort and cohorts stratified by patient age.</p><p><strong>Results: </strong>A total of 1517 patients met the study criteria; 33.8%, 35.5%, and 30.8% were aged < 65, 65-74, and ≥ 75 years, respectively. Exposure to ≥ 1 QTc-prolonging medication or ≥ 1 medication with known TdP risk was observed in 53.3% and 15.4% of patients at index, respectively, and 78.6% and 57.1% of patients during follow-up, respectively. Patients were exposed to QTc-prolonging medications for 54.6% of total person-time during follow-up. Patients aged ≥ 65 years had higher exposure to medications with conditional TdP risk than those aged < 65 years, primarily driven by increased diuretic use.</p><p><strong>Conclusions: </strong>QTc-prolonging medication use was common in patients with HR+/HER2- mBC receiving 1L CDK4/6i plus AI treatment, highlighting the importance of reviewing concomitant medications to inform CDK4/6i selection and patient monitoring while on treatment.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"64"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231290/pdf/","citationCount":"0","resultStr":"{\"title\":\"QT STAR: concomitant QTc-prolonging medication use among patients with HR+/HER2- metastatic breast cancer receiving a CDK4/6 inhibitor in first line.\",\"authors\":\"Susan Dent, Heather Moore, Michael Fradley, Chloe Grace Rose, Stella Stergiopoulos, Connie Chen, Benjamin Li, Avirup Guha\",\"doi\":\"10.1186/s40959-025-00364-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The risk of drug-induced corrected QT interval (QTc) prolongation is an important consideration in clinical decision-making for patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) metastatic breast cancer (mBC). This retrospective analysis described concomitant QTc-prolonging medication use in patients with HR+/HER2- mBC who received first-line (1L) treatment with a cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus an aromatase inhibitor (AI).</p><p><strong>Methods: </strong>This retrospective claims analysis utilized the Optum Clinformatics Data Mart database to identify patients with HR+/HER2- mBC who initiated 1L CDK4/6i plus AI treatment between January 2017 and March 2022. Exposure to QTc-prolonging medications (overall and by Torsades de Pointes [TdP] risk, per www.crediblemeds.org ) was assessed at index (i.e., CDK4/6i treatment initiation) and during follow-up (i.e., duration of CDK4/6i treatment) in the overall cohort and cohorts stratified by patient age.</p><p><strong>Results: </strong>A total of 1517 patients met the study criteria; 33.8%, 35.5%, and 30.8% were aged < 65, 65-74, and ≥ 75 years, respectively. Exposure to ≥ 1 QTc-prolonging medication or ≥ 1 medication with known TdP risk was observed in 53.3% and 15.4% of patients at index, respectively, and 78.6% and 57.1% of patients during follow-up, respectively. Patients were exposed to QTc-prolonging medications for 54.6% of total person-time during follow-up. Patients aged ≥ 65 years had higher exposure to medications with conditional TdP risk than those aged < 65 years, primarily driven by increased diuretic use.</p><p><strong>Conclusions: </strong>QTc-prolonging medication use was common in patients with HR+/HER2- mBC receiving 1L CDK4/6i plus AI treatment, highlighting the importance of reviewing concomitant medications to inform CDK4/6i selection and patient monitoring while on treatment.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"11 1\",\"pages\":\"64\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-07-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12231290/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-025-00364-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00364-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:药物诱导的纠正QT间期(QTc)延长的风险是激素受体阳性/人表皮生长因子受体2阴性(HR+/HER2-)转移性乳腺癌(mBC)患者临床决策的重要考虑因素。这项回顾性分析描述了HR+/HER2- mBC患者在接受周期蛋白依赖性激酶4/6抑制剂(CDK4/6i)和芳香酶抑制剂(AI)的一线(1L)治疗时同时使用延长qtc的药物。方法:利用Optum Clinformatics Data Mart数据库进行回顾性索赔分析,确定2017年1月至2022年3月期间接受1L CDK4/6i + AI治疗的HR+/HER2- mBC患者。在整个队列和按患者年龄分层的队列中,对延长qtc的药物暴露(总体和通过Torsades de Pointes [TdP]风险,按www.crediblemeds.org)的指标(即CDK4/6i治疗开始)和随访期间(即CDK4/6i治疗持续时间)进行评估。结果:1517例患者符合研究标准;结论:在接受1L CDK4/6i + AI治疗的HR+/HER2- mBC患者中,qtc延长用药是常见的,强调了在治疗过程中回顾伴随用药以指导CDK4/6i选择和患者监测的重要性。
QT STAR: concomitant QTc-prolonging medication use among patients with HR+/HER2- metastatic breast cancer receiving a CDK4/6 inhibitor in first line.
Background: The risk of drug-induced corrected QT interval (QTc) prolongation is an important consideration in clinical decision-making for patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2-) metastatic breast cancer (mBC). This retrospective analysis described concomitant QTc-prolonging medication use in patients with HR+/HER2- mBC who received first-line (1L) treatment with a cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) plus an aromatase inhibitor (AI).
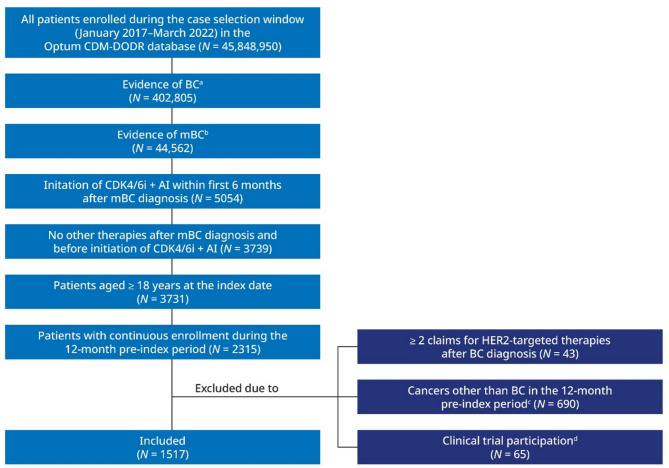
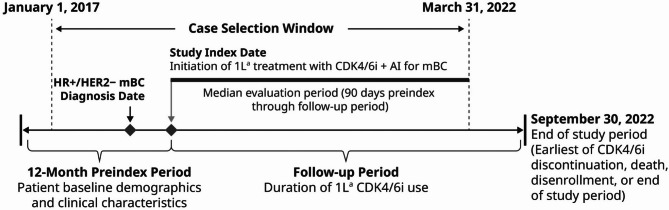
Methods: This retrospective claims analysis utilized the Optum Clinformatics Data Mart database to identify patients with HR+/HER2- mBC who initiated 1L CDK4/6i plus AI treatment between January 2017 and March 2022. Exposure to QTc-prolonging medications (overall and by Torsades de Pointes [TdP] risk, per www.crediblemeds.org ) was assessed at index (i.e., CDK4/6i treatment initiation) and during follow-up (i.e., duration of CDK4/6i treatment) in the overall cohort and cohorts stratified by patient age.
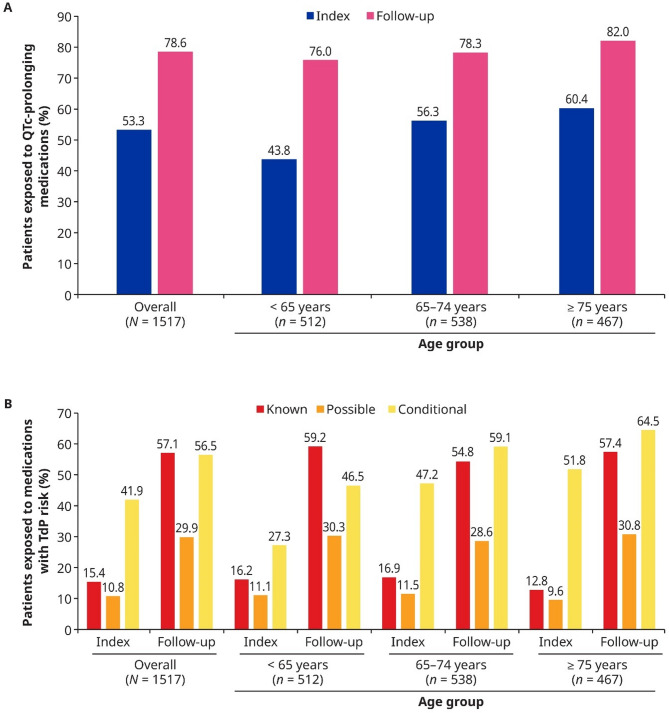
Results: A total of 1517 patients met the study criteria; 33.8%, 35.5%, and 30.8% were aged < 65, 65-74, and ≥ 75 years, respectively. Exposure to ≥ 1 QTc-prolonging medication or ≥ 1 medication with known TdP risk was observed in 53.3% and 15.4% of patients at index, respectively, and 78.6% and 57.1% of patients during follow-up, respectively. Patients were exposed to QTc-prolonging medications for 54.6% of total person-time during follow-up. Patients aged ≥ 65 years had higher exposure to medications with conditional TdP risk than those aged < 65 years, primarily driven by increased diuretic use.
Conclusions: QTc-prolonging medication use was common in patients with HR+/HER2- mBC receiving 1L CDK4/6i plus AI treatment, highlighting the importance of reviewing concomitant medications to inform CDK4/6i selection and patient monitoring while on treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


