Pedro Jallad, Marilia Soliani, Pedro Henrique Almeida Marins, Fábio Fernandes, Edmundo Arteaga-Fernandez, Vagner Madrini, Pedro Lemos Neto, Charles Mady, Felix Ramires, Alexandre A Abizaid, Fábio Sândoli de Brito, Henrique Barbosa Ribeiro
{"title":"酒精室间隔消融术治疗症状性肥厚性梗阻性心肌病的巴西多中心登记- BRASA登记","authors":"Pedro Jallad, Marilia Soliani, Pedro Henrique Almeida Marins, Fábio Fernandes, Edmundo Arteaga-Fernandez, Vagner Madrini, Pedro Lemos Neto, Charles Mady, Felix Ramires, Alexandre A Abizaid, Fábio Sândoli de Brito, Henrique Barbosa Ribeiro","doi":"10.36660/abc.20240626","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alcohol septal ablation (ASA) is an alternative to surgical myectomy for patients with symptomatic hypertrophic obstructive cardiomyopathy (HOCM) and significant left ventricular (LV) outflow tract (LVOT) obstruction. Although widely studied worldwide, data on ASA outcomes in Brazil are still limited.</p><p><strong>Objective: </strong>To assess the safety and effectiveness of ASA in symptomatic HOCM patients receiving optimal medical therapy using current techniques across multiple centers in Brazil.</p><p><strong>Methods: </strong>Patients with HOCM and angina (classified by the Canadian Cardiovascular Society [CCS]) or dyspnea (classified by the New York Heart Association [NYHA]) class >II who did not respond to optimal medical treatment were included. The primary efficacy endpoint was defined as a reduction of more than 50% in the maximum resting LVOT gradient, with a final gradient <50 mmHg. Patients were classified as responders or nonresponders. A p-value <0.05 was considered statistically significant.</p><p><strong>Results: </strong>A total of 41 patients (median age 66.4 years; 73% female) underwent ASA. At baseline, 93.2% were in NYHA class III/IV or CCS class III/IV. The mean LV ejection fraction (LVEF) was 66.4%, and the mean LVOT gradient was 88.4 mmHg. After 12 months, 92.8% had improved to NYHA class I/II or CCS class I/II (p<0.01). The mean LVOT gradient dropped from 88.4 mmHg to 27.0 mmHg (p=0.003), and interventricular septum (IVS) thickness decreased from 19.3 mm to 14.7 mm (p=0.048). Responders had lower baseline gradients (73.4 vs 112.6 mmHg, p=0.04) and fewer hospitalizations (21.1% vs 82.4%, p=0.04). Complete atrioventricular block occurred in 16.7% of patients, and 4.8% required pacemakers. No deaths were reported during a median follow-up of 394 days. At the last in-person evaluation, 78.4% were in functional class I/II.</p><p><strong>Conclusions: </strong>ASA is a safe, effective option for relieving symptoms in selected HOCM patients. It reduces LVOT gradient and septal thickness. Patients with higher baseline gradients were less likely to respond to the procedure.</p>","PeriodicalId":93887,"journal":{"name":"Arquivos brasileiros de cardiologia","volume":"122 6","pages":"e20240626"},"PeriodicalIF":1.9000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212378/pdf/","citationCount":"0","resultStr":"{\"title\":\"Brazilian Multicenter Registry of Alcohol Septal Ablation for Patients with Symptomatic Hypertrophic Obstructive Cardiomyopathy - BRASA Registry.\",\"authors\":\"Pedro Jallad, Marilia Soliani, Pedro Henrique Almeida Marins, Fábio Fernandes, Edmundo Arteaga-Fernandez, Vagner Madrini, Pedro Lemos Neto, Charles Mady, Felix Ramires, Alexandre A Abizaid, Fábio Sândoli de Brito, Henrique Barbosa Ribeiro\",\"doi\":\"10.36660/abc.20240626\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Alcohol septal ablation (ASA) is an alternative to surgical myectomy for patients with symptomatic hypertrophic obstructive cardiomyopathy (HOCM) and significant left ventricular (LV) outflow tract (LVOT) obstruction. Although widely studied worldwide, data on ASA outcomes in Brazil are still limited.</p><p><strong>Objective: </strong>To assess the safety and effectiveness of ASA in symptomatic HOCM patients receiving optimal medical therapy using current techniques across multiple centers in Brazil.</p><p><strong>Methods: </strong>Patients with HOCM and angina (classified by the Canadian Cardiovascular Society [CCS]) or dyspnea (classified by the New York Heart Association [NYHA]) class >II who did not respond to optimal medical treatment were included. The primary efficacy endpoint was defined as a reduction of more than 50% in the maximum resting LVOT gradient, with a final gradient <50 mmHg. Patients were classified as responders or nonresponders. A p-value <0.05 was considered statistically significant.</p><p><strong>Results: </strong>A total of 41 patients (median age 66.4 years; 73% female) underwent ASA. At baseline, 93.2% were in NYHA class III/IV or CCS class III/IV. The mean LV ejection fraction (LVEF) was 66.4%, and the mean LVOT gradient was 88.4 mmHg. After 12 months, 92.8% had improved to NYHA class I/II or CCS class I/II (p<0.01). The mean LVOT gradient dropped from 88.4 mmHg to 27.0 mmHg (p=0.003), and interventricular septum (IVS) thickness decreased from 19.3 mm to 14.7 mm (p=0.048). Responders had lower baseline gradients (73.4 vs 112.6 mmHg, p=0.04) and fewer hospitalizations (21.1% vs 82.4%, p=0.04). Complete atrioventricular block occurred in 16.7% of patients, and 4.8% required pacemakers. No deaths were reported during a median follow-up of 394 days. At the last in-person evaluation, 78.4% were in functional class I/II.</p><p><strong>Conclusions: </strong>ASA is a safe, effective option for relieving symptoms in selected HOCM patients. It reduces LVOT gradient and septal thickness. Patients with higher baseline gradients were less likely to respond to the procedure.</p>\",\"PeriodicalId\":93887,\"journal\":{\"name\":\"Arquivos brasileiros de cardiologia\",\"volume\":\"122 6\",\"pages\":\"e20240626\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212378/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arquivos brasileiros de cardiologia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36660/abc.20240626\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arquivos brasileiros de cardiologia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36660/abc.20240626","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
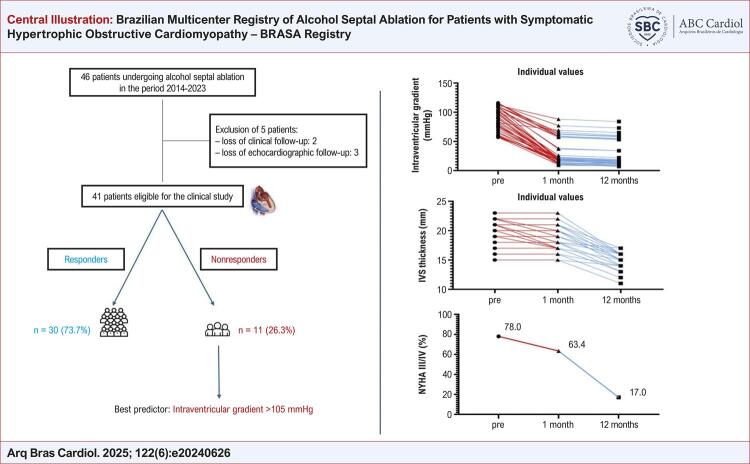
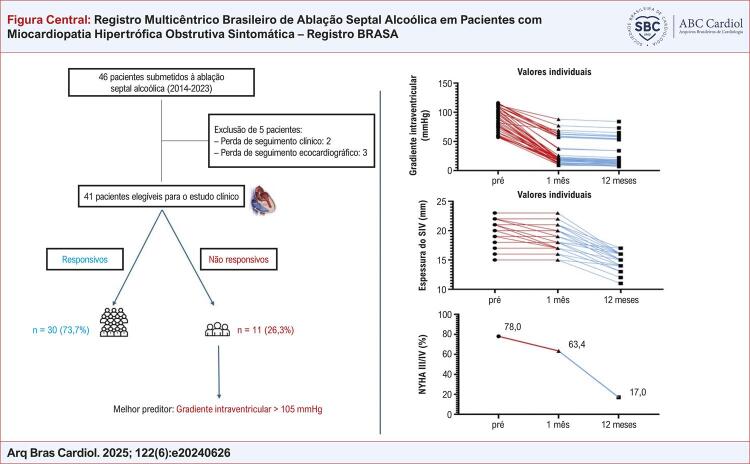
Brazilian Multicenter Registry of Alcohol Septal Ablation for Patients with Symptomatic Hypertrophic Obstructive Cardiomyopathy - BRASA Registry.
Background: Alcohol septal ablation (ASA) is an alternative to surgical myectomy for patients with symptomatic hypertrophic obstructive cardiomyopathy (HOCM) and significant left ventricular (LV) outflow tract (LVOT) obstruction. Although widely studied worldwide, data on ASA outcomes in Brazil are still limited.
Objective: To assess the safety and effectiveness of ASA in symptomatic HOCM patients receiving optimal medical therapy using current techniques across multiple centers in Brazil.
Methods: Patients with HOCM and angina (classified by the Canadian Cardiovascular Society [CCS]) or dyspnea (classified by the New York Heart Association [NYHA]) class >II who did not respond to optimal medical treatment were included. The primary efficacy endpoint was defined as a reduction of more than 50% in the maximum resting LVOT gradient, with a final gradient <50 mmHg. Patients were classified as responders or nonresponders. A p-value <0.05 was considered statistically significant.
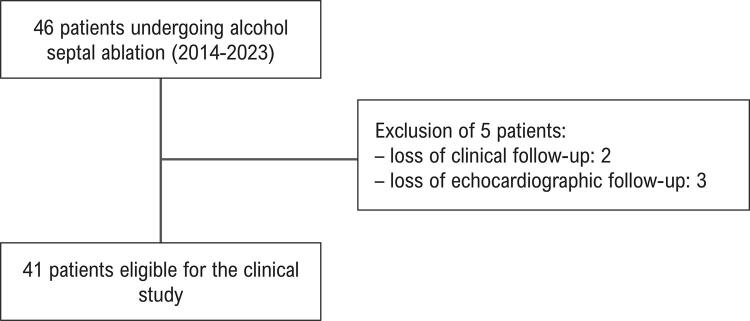
Results: A total of 41 patients (median age 66.4 years; 73% female) underwent ASA. At baseline, 93.2% were in NYHA class III/IV or CCS class III/IV. The mean LV ejection fraction (LVEF) was 66.4%, and the mean LVOT gradient was 88.4 mmHg. After 12 months, 92.8% had improved to NYHA class I/II or CCS class I/II (p<0.01). The mean LVOT gradient dropped from 88.4 mmHg to 27.0 mmHg (p=0.003), and interventricular septum (IVS) thickness decreased from 19.3 mm to 14.7 mm (p=0.048). Responders had lower baseline gradients (73.4 vs 112.6 mmHg, p=0.04) and fewer hospitalizations (21.1% vs 82.4%, p=0.04). Complete atrioventricular block occurred in 16.7% of patients, and 4.8% required pacemakers. No deaths were reported during a median follow-up of 394 days. At the last in-person evaluation, 78.4% were in functional class I/II.
Conclusions: ASA is a safe, effective option for relieving symptoms in selected HOCM patients. It reduces LVOT gradient and septal thickness. Patients with higher baseline gradients were less likely to respond to the procedure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


