Raja Zaghlol, Elena Deych, Nina Manian, Ahmed Altibi, Joshua D Mitchell
{"title":"在美国全国范围内进行干细胞移植患者的心房颤动或扑动,住院和出院后的结果","authors":"Raja Zaghlol, Elena Deych, Nina Manian, Ahmed Altibi, Joshua D Mitchell","doi":"10.1186/s40959-025-00346-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Stem Cell Transplantation (SCT) is a cornerstone therapy in managing several malignant and benign hematological conditions. Atrial fibrillation/atrial flutter (AF) are commonly encountered in patients receiving SCT. There is a paucity of large-scale data on the prevalence of AF and their effect on outcomes following SCT.</p><p><strong>Methods: </strong>The United States National Readmission Database (NRD) was used to identify hospitalized patients who underwent SCT. Baseline demographics, comorbidities, the presence or absence of AF, the indication, and type of SCT were identified using diagnostic and procedural International Classification of Diseases 10th Edition (ICD-10) codes. Patients with AF were compared to those without AF for differences in baseline characteristics, in-hospital mortality, cardiovascular (CV) complications, length and cost of hospitalization, and post-discharge 90-day readmissions and mortality.</p><p><strong>Results: </strong>Between January 2016 and September 2020 there were 59,284 weighted admissions for SCT, of which 5797 (9.8%) patients had AF. Patients in the AF group were more likely to be older males with an increased burden of baseline comorbidities compared to the no-AF group ((64 [9] vs. 56 [14] years, p < 0.001) and (3893 [67%] vs. 30,886 [58%] males, p < 0.001) respectively). Adjusted for differences in baseline demographics, comorbidities, indication and type of SCT, patients with AF had higher in-hospital mortality (adjusted odds ratio (AOR) 3.65 [3.02-4.41]) and adverse events including cardiac complications [composite of acute heart failure, acute myocardial infarction, cardiogenic shock, and cardiac arrest] (AOR 4.92 [4.22-5.75]), bleeding (AOR 1.32 [1.15-1.53]), and respiratory failure (AOR 3.40 [2.97-3.90]) compared to patients without AF. Additionally, the AF group had longer hospitalizations (21 [16-27] vs. 19 [15-25] days, p < 0.001) with higher cost ($268,031 [$170,957-$455739] vs. $250,178 [$153,680-$415239], p < 0.001) compared to the no-AF group. Among survivors to hospital discharge, patients with AF also had higher adjusted 90-day all-cause inpatient mortality (adjusted hazard ratio (AHR) 1.54 [1.19-1.99], p = 0.001), all-cause readmissions (AHR 1.15 [1.07-1.24], p < 0.001), and CV readmissions (AHR 2.29 [1.85-2.82], p < 0.001).</p><p><strong>Conclusions: </strong>In a large national cohort of SCT recipients, AF were common and independently associated with increased in-hospital mortality and CV adverse events, along with increased 90-day mortality and readmissions among survivors to hospital discharge.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"61"},"PeriodicalIF":3.2000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225381/pdf/","citationCount":"0","resultStr":"{\"title\":\"Atrial fibrillation or flutter in patients undergoing stem cell transplantation, in-hospital and post-discharge outcomes in a large nationwide sample across the United States.\",\"authors\":\"Raja Zaghlol, Elena Deych, Nina Manian, Ahmed Altibi, Joshua D Mitchell\",\"doi\":\"10.1186/s40959-025-00346-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Stem Cell Transplantation (SCT) is a cornerstone therapy in managing several malignant and benign hematological conditions. Atrial fibrillation/atrial flutter (AF) are commonly encountered in patients receiving SCT. There is a paucity of large-scale data on the prevalence of AF and their effect on outcomes following SCT.</p><p><strong>Methods: </strong>The United States National Readmission Database (NRD) was used to identify hospitalized patients who underwent SCT. Baseline demographics, comorbidities, the presence or absence of AF, the indication, and type of SCT were identified using diagnostic and procedural International Classification of Diseases 10th Edition (ICD-10) codes. Patients with AF were compared to those without AF for differences in baseline characteristics, in-hospital mortality, cardiovascular (CV) complications, length and cost of hospitalization, and post-discharge 90-day readmissions and mortality.</p><p><strong>Results: </strong>Between January 2016 and September 2020 there were 59,284 weighted admissions for SCT, of which 5797 (9.8%) patients had AF. Patients in the AF group were more likely to be older males with an increased burden of baseline comorbidities compared to the no-AF group ((64 [9] vs. 56 [14] years, p < 0.001) and (3893 [67%] vs. 30,886 [58%] males, p < 0.001) respectively). Adjusted for differences in baseline demographics, comorbidities, indication and type of SCT, patients with AF had higher in-hospital mortality (adjusted odds ratio (AOR) 3.65 [3.02-4.41]) and adverse events including cardiac complications [composite of acute heart failure, acute myocardial infarction, cardiogenic shock, and cardiac arrest] (AOR 4.92 [4.22-5.75]), bleeding (AOR 1.32 [1.15-1.53]), and respiratory failure (AOR 3.40 [2.97-3.90]) compared to patients without AF. Additionally, the AF group had longer hospitalizations (21 [16-27] vs. 19 [15-25] days, p < 0.001) with higher cost ($268,031 [$170,957-$455739] vs. $250,178 [$153,680-$415239], p < 0.001) compared to the no-AF group. Among survivors to hospital discharge, patients with AF also had higher adjusted 90-day all-cause inpatient mortality (adjusted hazard ratio (AHR) 1.54 [1.19-1.99], p = 0.001), all-cause readmissions (AHR 1.15 [1.07-1.24], p < 0.001), and CV readmissions (AHR 2.29 [1.85-2.82], p < 0.001).</p><p><strong>Conclusions: </strong>In a large national cohort of SCT recipients, AF were common and independently associated with increased in-hospital mortality and CV adverse events, along with increased 90-day mortality and readmissions among survivors to hospital discharge.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"11 1\",\"pages\":\"61\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-07-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225381/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-025-00346-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00346-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Atrial fibrillation or flutter in patients undergoing stem cell transplantation, in-hospital and post-discharge outcomes in a large nationwide sample across the United States.
Background: Stem Cell Transplantation (SCT) is a cornerstone therapy in managing several malignant and benign hematological conditions. Atrial fibrillation/atrial flutter (AF) are commonly encountered in patients receiving SCT. There is a paucity of large-scale data on the prevalence of AF and their effect on outcomes following SCT.
Methods: The United States National Readmission Database (NRD) was used to identify hospitalized patients who underwent SCT. Baseline demographics, comorbidities, the presence or absence of AF, the indication, and type of SCT were identified using diagnostic and procedural International Classification of Diseases 10th Edition (ICD-10) codes. Patients with AF were compared to those without AF for differences in baseline characteristics, in-hospital mortality, cardiovascular (CV) complications, length and cost of hospitalization, and post-discharge 90-day readmissions and mortality.
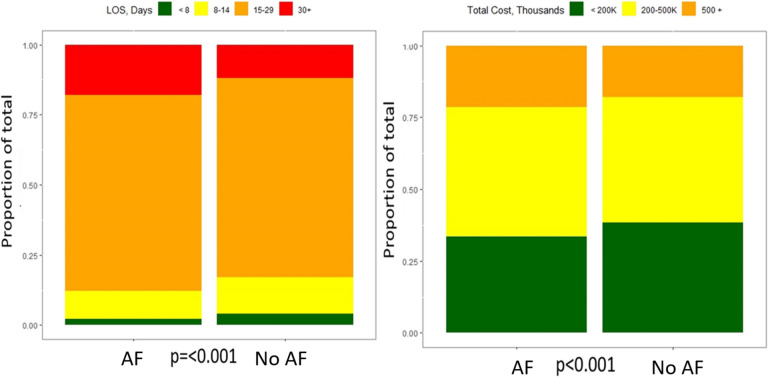
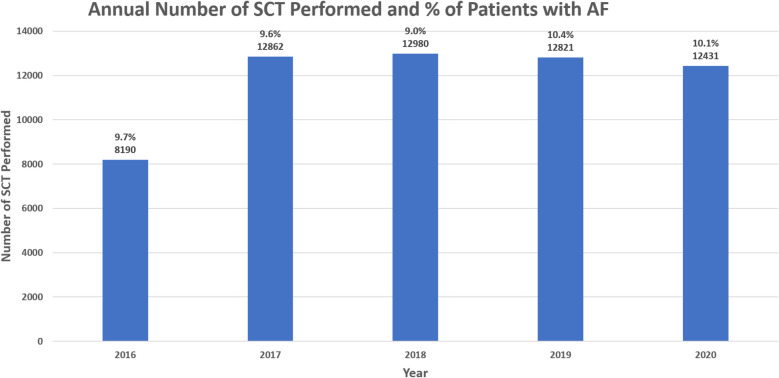
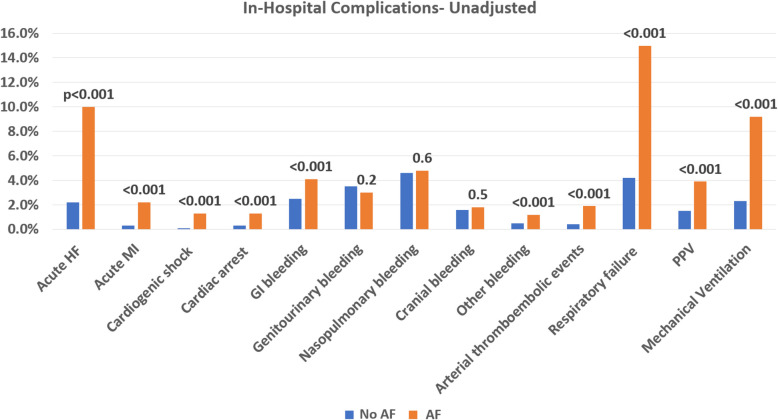
Results: Between January 2016 and September 2020 there were 59,284 weighted admissions for SCT, of which 5797 (9.8%) patients had AF. Patients in the AF group were more likely to be older males with an increased burden of baseline comorbidities compared to the no-AF group ((64 [9] vs. 56 [14] years, p < 0.001) and (3893 [67%] vs. 30,886 [58%] males, p < 0.001) respectively). Adjusted for differences in baseline demographics, comorbidities, indication and type of SCT, patients with AF had higher in-hospital mortality (adjusted odds ratio (AOR) 3.65 [3.02-4.41]) and adverse events including cardiac complications [composite of acute heart failure, acute myocardial infarction, cardiogenic shock, and cardiac arrest] (AOR 4.92 [4.22-5.75]), bleeding (AOR 1.32 [1.15-1.53]), and respiratory failure (AOR 3.40 [2.97-3.90]) compared to patients without AF. Additionally, the AF group had longer hospitalizations (21 [16-27] vs. 19 [15-25] days, p < 0.001) with higher cost ($268,031 [$170,957-$455739] vs. $250,178 [$153,680-$415239], p < 0.001) compared to the no-AF group. Among survivors to hospital discharge, patients with AF also had higher adjusted 90-day all-cause inpatient mortality (adjusted hazard ratio (AHR) 1.54 [1.19-1.99], p = 0.001), all-cause readmissions (AHR 1.15 [1.07-1.24], p < 0.001), and CV readmissions (AHR 2.29 [1.85-2.82], p < 0.001).
Conclusions: In a large national cohort of SCT recipients, AF were common and independently associated with increased in-hospital mortality and CV adverse events, along with increased 90-day mortality and readmissions among survivors to hospital discharge.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


