Lingyi Lu, Lu Cao, Fan Jiang, Sihan Wang, Yingzhe Yu, Hua Huang, Bingjiang Lin
{"title":"难治性身体部位银屑病的流行病学和临床特征:一项基于中国全国人群的研究。","authors":"Lingyi Lu, Lu Cao, Fan Jiang, Sihan Wang, Yingzhe Yu, Hua Huang, Bingjiang Lin","doi":"10.1186/s12865-025-00724-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Having psoriasis in hard-to-treat areas, such as the scalp, face, palms, soles, nails, and genitals, can suffer from a reduced quality of life. This study was designed to investigate the prevalence and risk factors of hard-to-treat body locations of psoriasis, and to describe patients' clinical and demographic characteristics, and quality of life impacts.</p><p><strong>Methods: </strong>We conducted a multicenter observational epidemiological study involving over 1000 hospitals in China, enrolling a total of 7032 psoriasis patients. Groups were compared to patients without involvement of hard-to-treat areas.</p><p><strong>Results: </strong>The most frequently affected hard-to-treat area was the scalp (60.01%), followed by the face (22.47%), nails (18.87%), palms or soles (18.23%), genitals or vulvas (12.00%), respectively. Among all patients, 70.71%, 36.65%, 16.30%, 6.48% and 1.45% of patients had involvement of ≥ 1, ≥2, ≥ 3, ≥4 or ≥ 5 hard-to-treat areas. There was a male predominance among patients with involvement of at least one hard-to-treat area(P < 0.001). The smoking rate, BMI (body mass index) and psoriasis family history in patients with at least one hard-to-treat area involvement were significantly higher than those in patients without hard-to-treat area involvement (P < 0.001), especially among patients with nail involvement. With regards to current DLQI (dermatology life quality index), satisfactory rate, and current BSA (body surface area), these findings were all significantly different (P < 0.001) when compared to patients without involvement of a hard-to-treat area. Notably, even in mild-to-moderate psoriasis (BSA < 10), 65.10% of patients showed involvement of ≥ 1 hard-to-treat area, with significant impacts on quality of life (DLQI increase, all P < 0.001) and treatment satisfaction (P < 0.001 vs. non-involved).</p><p><strong>Conclusion: </strong>Psoriasis commonly affects hard-to-treat locations, even in patients with mild to moderate disease (BSA < 10). The disproportionate impact on quality of life (particularly genital/face involvement) and treatment satisfaction underscores the need for: (1) routine assessment of these areas regardless of BSA, and (2) targeted management of modifiable risk factors (smoking, obesity). These findings support incorporating hard-to-treat area evaluation into psoriasis severity assessments and treatment algorithms.</p>","PeriodicalId":9040,"journal":{"name":"BMC Immunology","volume":"26 1","pages":"45"},"PeriodicalIF":2.7000,"publicationDate":"2025-07-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225188/pdf/","citationCount":"0","resultStr":"{\"title\":\"Epidemiology and clinical features of psoriasis in hard-to-treat body locations: a Chinese nationwide population-based study.\",\"authors\":\"Lingyi Lu, Lu Cao, Fan Jiang, Sihan Wang, Yingzhe Yu, Hua Huang, Bingjiang Lin\",\"doi\":\"10.1186/s12865-025-00724-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Having psoriasis in hard-to-treat areas, such as the scalp, face, palms, soles, nails, and genitals, can suffer from a reduced quality of life. This study was designed to investigate the prevalence and risk factors of hard-to-treat body locations of psoriasis, and to describe patients' clinical and demographic characteristics, and quality of life impacts.</p><p><strong>Methods: </strong>We conducted a multicenter observational epidemiological study involving over 1000 hospitals in China, enrolling a total of 7032 psoriasis patients. Groups were compared to patients without involvement of hard-to-treat areas.</p><p><strong>Results: </strong>The most frequently affected hard-to-treat area was the scalp (60.01%), followed by the face (22.47%), nails (18.87%), palms or soles (18.23%), genitals or vulvas (12.00%), respectively. Among all patients, 70.71%, 36.65%, 16.30%, 6.48% and 1.45% of patients had involvement of ≥ 1, ≥2, ≥ 3, ≥4 or ≥ 5 hard-to-treat areas. There was a male predominance among patients with involvement of at least one hard-to-treat area(P < 0.001). The smoking rate, BMI (body mass index) and psoriasis family history in patients with at least one hard-to-treat area involvement were significantly higher than those in patients without hard-to-treat area involvement (P < 0.001), especially among patients with nail involvement. With regards to current DLQI (dermatology life quality index), satisfactory rate, and current BSA (body surface area), these findings were all significantly different (P < 0.001) when compared to patients without involvement of a hard-to-treat area. Notably, even in mild-to-moderate psoriasis (BSA < 10), 65.10% of patients showed involvement of ≥ 1 hard-to-treat area, with significant impacts on quality of life (DLQI increase, all P < 0.001) and treatment satisfaction (P < 0.001 vs. non-involved).</p><p><strong>Conclusion: </strong>Psoriasis commonly affects hard-to-treat locations, even in patients with mild to moderate disease (BSA < 10). The disproportionate impact on quality of life (particularly genital/face involvement) and treatment satisfaction underscores the need for: (1) routine assessment of these areas regardless of BSA, and (2) targeted management of modifiable risk factors (smoking, obesity). These findings support incorporating hard-to-treat area evaluation into psoriasis severity assessments and treatment algorithms.</p>\",\"PeriodicalId\":9040,\"journal\":{\"name\":\"BMC Immunology\",\"volume\":\"26 1\",\"pages\":\"45\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-07-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12225188/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Immunology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12865-025-00724-5\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Immunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12865-025-00724-5","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Epidemiology and clinical features of psoriasis in hard-to-treat body locations: a Chinese nationwide population-based study.
Background: Having psoriasis in hard-to-treat areas, such as the scalp, face, palms, soles, nails, and genitals, can suffer from a reduced quality of life. This study was designed to investigate the prevalence and risk factors of hard-to-treat body locations of psoriasis, and to describe patients' clinical and demographic characteristics, and quality of life impacts.
Methods: We conducted a multicenter observational epidemiological study involving over 1000 hospitals in China, enrolling a total of 7032 psoriasis patients. Groups were compared to patients without involvement of hard-to-treat areas.
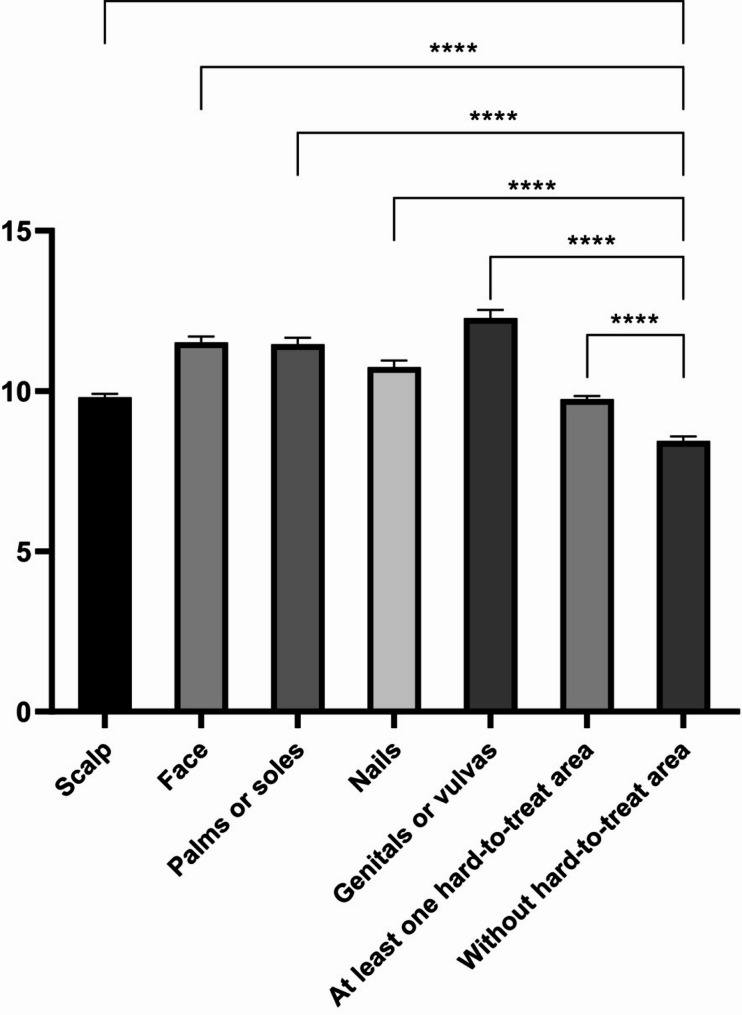
Results: The most frequently affected hard-to-treat area was the scalp (60.01%), followed by the face (22.47%), nails (18.87%), palms or soles (18.23%), genitals or vulvas (12.00%), respectively. Among all patients, 70.71%, 36.65%, 16.30%, 6.48% and 1.45% of patients had involvement of ≥ 1, ≥2, ≥ 3, ≥4 or ≥ 5 hard-to-treat areas. There was a male predominance among patients with involvement of at least one hard-to-treat area(P < 0.001). The smoking rate, BMI (body mass index) and psoriasis family history in patients with at least one hard-to-treat area involvement were significantly higher than those in patients without hard-to-treat area involvement (P < 0.001), especially among patients with nail involvement. With regards to current DLQI (dermatology life quality index), satisfactory rate, and current BSA (body surface area), these findings were all significantly different (P < 0.001) when compared to patients without involvement of a hard-to-treat area. Notably, even in mild-to-moderate psoriasis (BSA < 10), 65.10% of patients showed involvement of ≥ 1 hard-to-treat area, with significant impacts on quality of life (DLQI increase, all P < 0.001) and treatment satisfaction (P < 0.001 vs. non-involved).
Conclusion: Psoriasis commonly affects hard-to-treat locations, even in patients with mild to moderate disease (BSA < 10). The disproportionate impact on quality of life (particularly genital/face involvement) and treatment satisfaction underscores the need for: (1) routine assessment of these areas regardless of BSA, and (2) targeted management of modifiable risk factors (smoking, obesity). These findings support incorporating hard-to-treat area evaluation into psoriasis severity assessments and treatment algorithms.
期刊介绍:
BMC Immunology is an open access journal publishing original peer-reviewed research articles in molecular, cellular, tissue-level, organismal, functional, and developmental aspects of the immune system as well as clinical studies and animal models of human diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


