Cornelius J Fernandez, Vijaya Lakshmi, Abul Bashar M Kamrul-Hasan, Joseph M Pappachan
{"title":"肢端肥大症垂体瘤切除术后影响疾病控制的因素:目前的证据是什么?","authors":"Cornelius J Fernandez, Vijaya Lakshmi, Abul Bashar M Kamrul-Hasan, Joseph M Pappachan","doi":"10.4329/wjr.v17.i6.106438","DOIUrl":null,"url":null,"abstract":"<p><p>Acromegaly, characterized by persistent hypersecretion of growth hormone (GH), is most often caused by a pituitary neuroendocrine tumor (PitNET), though, less often, ectopic GH or GH-releasing hormone secretion from various neoplasms outside the pituitary gland could cause it. Nearly 70% of somatotroph PitNETs are macroadenomas at diagnosis. Transsphenoidal surgery, the most effective treatment modality for acromegaly, could achieve remission in 73%. However, the remission rates could reach 87% if surgery is followed by medical therapy. Due to variable therapeutic responses to surgical and medical therapy, pre-treatment awareness regarding the best therapeutic modality based on clinical, biochemical, radiological, histopathological and genetic parameters would help in accurate pretreatment decision-making. Earlier studies have identified poor prognosis markers like tumor size, tumor invasion, T2-weighted hyperintensity, granulation, and pretreatment GH and/or insulin-like growth factor 1 levels. In a recent study, published by Alvarez <i>et al</i> identified that preoperative PitNET volume is a good predictor of control of acromegaly following surgical treatment and the likelihood of requiring more aggressive additional therapies after surgery. They found that PitNET volume exceeding 3697 mm³ was associated with poorer disease control in patients with somatotroph PitNETs.</p>","PeriodicalId":23819,"journal":{"name":"World journal of radiology","volume":"17 6","pages":"106438"},"PeriodicalIF":1.5000,"publicationDate":"2025-06-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12210195/pdf/","citationCount":"0","resultStr":"{\"title\":\"Factors affecting disease control after pituitary tumor resection in acromegaly: What is the current evidence?\",\"authors\":\"Cornelius J Fernandez, Vijaya Lakshmi, Abul Bashar M Kamrul-Hasan, Joseph M Pappachan\",\"doi\":\"10.4329/wjr.v17.i6.106438\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Acromegaly, characterized by persistent hypersecretion of growth hormone (GH), is most often caused by a pituitary neuroendocrine tumor (PitNET), though, less often, ectopic GH or GH-releasing hormone secretion from various neoplasms outside the pituitary gland could cause it. Nearly 70% of somatotroph PitNETs are macroadenomas at diagnosis. Transsphenoidal surgery, the most effective treatment modality for acromegaly, could achieve remission in 73%. However, the remission rates could reach 87% if surgery is followed by medical therapy. Due to variable therapeutic responses to surgical and medical therapy, pre-treatment awareness regarding the best therapeutic modality based on clinical, biochemical, radiological, histopathological and genetic parameters would help in accurate pretreatment decision-making. Earlier studies have identified poor prognosis markers like tumor size, tumor invasion, T2-weighted hyperintensity, granulation, and pretreatment GH and/or insulin-like growth factor 1 levels. In a recent study, published by Alvarez <i>et al</i> identified that preoperative PitNET volume is a good predictor of control of acromegaly following surgical treatment and the likelihood of requiring more aggressive additional therapies after surgery. They found that PitNET volume exceeding 3697 mm³ was associated with poorer disease control in patients with somatotroph PitNETs.</p>\",\"PeriodicalId\":23819,\"journal\":{\"name\":\"World journal of radiology\",\"volume\":\"17 6\",\"pages\":\"106438\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-06-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12210195/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4329/wjr.v17.i6.106438\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4329/wjr.v17.i6.106438","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Factors affecting disease control after pituitary tumor resection in acromegaly: What is the current evidence?
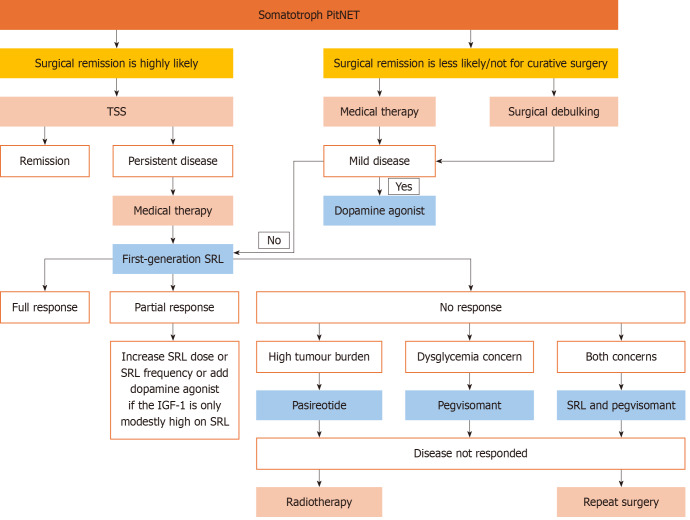
Acromegaly, characterized by persistent hypersecretion of growth hormone (GH), is most often caused by a pituitary neuroendocrine tumor (PitNET), though, less often, ectopic GH or GH-releasing hormone secretion from various neoplasms outside the pituitary gland could cause it. Nearly 70% of somatotroph PitNETs are macroadenomas at diagnosis. Transsphenoidal surgery, the most effective treatment modality for acromegaly, could achieve remission in 73%. However, the remission rates could reach 87% if surgery is followed by medical therapy. Due to variable therapeutic responses to surgical and medical therapy, pre-treatment awareness regarding the best therapeutic modality based on clinical, biochemical, radiological, histopathological and genetic parameters would help in accurate pretreatment decision-making. Earlier studies have identified poor prognosis markers like tumor size, tumor invasion, T2-weighted hyperintensity, granulation, and pretreatment GH and/or insulin-like growth factor 1 levels. In a recent study, published by Alvarez et al identified that preoperative PitNET volume is a good predictor of control of acromegaly following surgical treatment and the likelihood of requiring more aggressive additional therapies after surgery. They found that PitNET volume exceeding 3697 mm³ was associated with poorer disease control in patients with somatotroph PitNETs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


