Allison D Ta, Jonathan R Dillman, Nicholas J Ollberding, Yael Haberman, Robert Baldassano, James Markowitz, Anthony Otley, Jennifer L Dotson, Marian Pfefferkorn, Jeffrey S Hyams, Melvin B Heyman, Sandra C Kim, Joshua Noe, Scott Snapper, Adina Alazraki, Subra Kugathasan, Lee A Denson
{"title":"基线终末回肠CT和MRI测量与儿童克罗恩病的成像结果相关:一项队列研究","authors":"Allison D Ta, Jonathan R Dillman, Nicholas J Ollberding, Yael Haberman, Robert Baldassano, James Markowitz, Anthony Otley, Jennifer L Dotson, Marian Pfefferkorn, Jeffrey S Hyams, Melvin B Heyman, Sandra C Kim, Joshua Noe, Scott Snapper, Adina Alazraki, Subra Kugathasan, Lee A Denson","doi":"10.1007/s00247-025-06302-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cross-sectional imaging is increasingly used for both initial diagnosis and long-term monitoring of Crohn's disease. The quantitative morphology of the terminal ileum may predict treatment response.</p><p><strong>Objective: </strong>We aimed to identify baseline qualitative and quantitative imaging features that are associated with clinical and radiologic treatment response in a large cohort of children with Crohn's disease.</p><p><strong>Materials and methods: </strong>This was a retrospective study of the RISK cohort study in pediatric Crohn's disease. This multicenter study included 1,136 children <18 years from 28 sites in North America. Subjects enrolled with newly diagnosed Crohn's disease who underwent endoscopy with baseline and follow-up CT or MRI were considered for this study. Exclusion criteria were incomplete data or surgical resection prior to follow-up imaging. Imaging analysis included assessing a qualitative terminal ileum (TI) categorical score based on SAR-AGA consensus definitions ((1) normal, (2) inflammation only without luminal narrowing, (3) inflammation with luminal narrowing, or (4) stricture with pre-stenotic dilation ≥3 cm) and quantitative measurements (maximum bowel wall thickness and maximum/minimum lumen diameter). Two endpoints were considered: (1) clinical response (off corticosteroids and quiescent Physician Global Assessment at follow-up imaging) and (2) CT and MRI response (follow-up imaging normalization). Multivariable logistic regression analyses were developed for each endpoint.</p><p><strong>Results: </strong>Ninety-six subjects were included. Clinical response endpoint was achieved in 38% (n=36) of participants, and imaging normalization was achieved in only 20% (n=19) of participants. Follow-up imaging showed disease progression in 24 (25%) patients, 7 (7%) of whom were radiologically normal at baseline (7%). A higher baseline TI categorical score was associated with lower odds of imaging normalization during follow-up (OR 0.4 [0.2, 0.8], P=0.009). Larger TI minimum lumen diameter (OR 1.1 [1.01, 1.3], P=0.04) and smaller maximum bowel wall thickness at baseline (OR 0.8 [0.6, 0.97], P=0.03) were associated with imaging normalization. There were no baseline imaging measurements associated with clinical response.</p><p><strong>Conclusions: </strong>Baseline increased terminal ileal minimum lumen diameter and decreasing wall thickness were associated with imaging normalization at follow-up, but not clinical response.</p>","PeriodicalId":19755,"journal":{"name":"Pediatric Radiology","volume":" ","pages":"1642-1651"},"PeriodicalIF":2.3000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12321652/pdf/","citationCount":"0","resultStr":"{\"title\":\"Baseline terminal ileal CT and MRI measurements are associated with imaging outcomes in pediatric Crohn's disease: a cohort study.\",\"authors\":\"Allison D Ta, Jonathan R Dillman, Nicholas J Ollberding, Yael Haberman, Robert Baldassano, James Markowitz, Anthony Otley, Jennifer L Dotson, Marian Pfefferkorn, Jeffrey S Hyams, Melvin B Heyman, Sandra C Kim, Joshua Noe, Scott Snapper, Adina Alazraki, Subra Kugathasan, Lee A Denson\",\"doi\":\"10.1007/s00247-025-06302-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cross-sectional imaging is increasingly used for both initial diagnosis and long-term monitoring of Crohn's disease. The quantitative morphology of the terminal ileum may predict treatment response.</p><p><strong>Objective: </strong>We aimed to identify baseline qualitative and quantitative imaging features that are associated with clinical and radiologic treatment response in a large cohort of children with Crohn's disease.</p><p><strong>Materials and methods: </strong>This was a retrospective study of the RISK cohort study in pediatric Crohn's disease. This multicenter study included 1,136 children <18 years from 28 sites in North America. Subjects enrolled with newly diagnosed Crohn's disease who underwent endoscopy with baseline and follow-up CT or MRI were considered for this study. Exclusion criteria were incomplete data or surgical resection prior to follow-up imaging. Imaging analysis included assessing a qualitative terminal ileum (TI) categorical score based on SAR-AGA consensus definitions ((1) normal, (2) inflammation only without luminal narrowing, (3) inflammation with luminal narrowing, or (4) stricture with pre-stenotic dilation ≥3 cm) and quantitative measurements (maximum bowel wall thickness and maximum/minimum lumen diameter). Two endpoints were considered: (1) clinical response (off corticosteroids and quiescent Physician Global Assessment at follow-up imaging) and (2) CT and MRI response (follow-up imaging normalization). Multivariable logistic regression analyses were developed for each endpoint.</p><p><strong>Results: </strong>Ninety-six subjects were included. Clinical response endpoint was achieved in 38% (n=36) of participants, and imaging normalization was achieved in only 20% (n=19) of participants. Follow-up imaging showed disease progression in 24 (25%) patients, 7 (7%) of whom were radiologically normal at baseline (7%). A higher baseline TI categorical score was associated with lower odds of imaging normalization during follow-up (OR 0.4 [0.2, 0.8], P=0.009). Larger TI minimum lumen diameter (OR 1.1 [1.01, 1.3], P=0.04) and smaller maximum bowel wall thickness at baseline (OR 0.8 [0.6, 0.97], P=0.03) were associated with imaging normalization. There were no baseline imaging measurements associated with clinical response.</p><p><strong>Conclusions: </strong>Baseline increased terminal ileal minimum lumen diameter and decreasing wall thickness were associated with imaging normalization at follow-up, but not clinical response.</p>\",\"PeriodicalId\":19755,\"journal\":{\"name\":\"Pediatric Radiology\",\"volume\":\" \",\"pages\":\"1642-1651\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12321652/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pediatric Radiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00247-025-06302-6\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00247-025-06302-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Baseline terminal ileal CT and MRI measurements are associated with imaging outcomes in pediatric Crohn's disease: a cohort study.
Background: Cross-sectional imaging is increasingly used for both initial diagnosis and long-term monitoring of Crohn's disease. The quantitative morphology of the terminal ileum may predict treatment response.
Objective: We aimed to identify baseline qualitative and quantitative imaging features that are associated with clinical and radiologic treatment response in a large cohort of children with Crohn's disease.
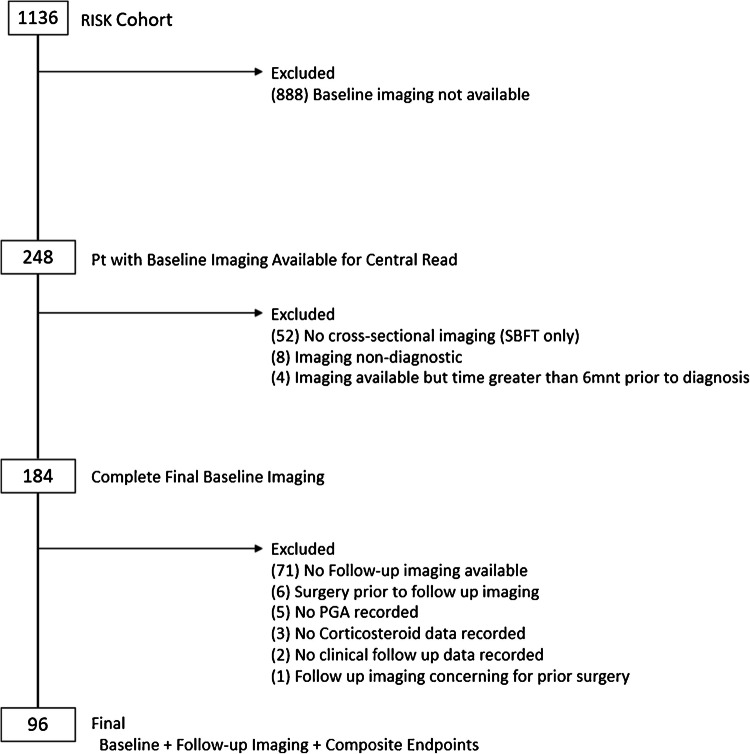
Materials and methods: This was a retrospective study of the RISK cohort study in pediatric Crohn's disease. This multicenter study included 1,136 children <18 years from 28 sites in North America. Subjects enrolled with newly diagnosed Crohn's disease who underwent endoscopy with baseline and follow-up CT or MRI were considered for this study. Exclusion criteria were incomplete data or surgical resection prior to follow-up imaging. Imaging analysis included assessing a qualitative terminal ileum (TI) categorical score based on SAR-AGA consensus definitions ((1) normal, (2) inflammation only without luminal narrowing, (3) inflammation with luminal narrowing, or (4) stricture with pre-stenotic dilation ≥3 cm) and quantitative measurements (maximum bowel wall thickness and maximum/minimum lumen diameter). Two endpoints were considered: (1) clinical response (off corticosteroids and quiescent Physician Global Assessment at follow-up imaging) and (2) CT and MRI response (follow-up imaging normalization). Multivariable logistic regression analyses were developed for each endpoint.
Results: Ninety-six subjects were included. Clinical response endpoint was achieved in 38% (n=36) of participants, and imaging normalization was achieved in only 20% (n=19) of participants. Follow-up imaging showed disease progression in 24 (25%) patients, 7 (7%) of whom were radiologically normal at baseline (7%). A higher baseline TI categorical score was associated with lower odds of imaging normalization during follow-up (OR 0.4 [0.2, 0.8], P=0.009). Larger TI minimum lumen diameter (OR 1.1 [1.01, 1.3], P=0.04) and smaller maximum bowel wall thickness at baseline (OR 0.8 [0.6, 0.97], P=0.03) were associated with imaging normalization. There were no baseline imaging measurements associated with clinical response.
Conclusions: Baseline increased terminal ileal minimum lumen diameter and decreasing wall thickness were associated with imaging normalization at follow-up, but not clinical response.
期刊介绍:
Official Journal of the European Society of Pediatric Radiology, the Society for Pediatric Radiology and the Asian and Oceanic Society for Pediatric Radiology
Pediatric Radiology informs its readers of new findings and progress in all areas of pediatric imaging and in related fields. This is achieved by a blend of original papers, complemented by reviews that set out the present state of knowledge in a particular area of the specialty or summarize specific topics in which discussion has led to clear conclusions. Advances in technology, methodology, apparatus and auxiliary equipment are presented, and modifications of standard techniques are described.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1964 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


