Thomas L Lewis, Sanjana Mehrotra, Jonathan Kaplan, Tyler Gonzalez, Sergio Morales, Thomas J Goff, Vikramman Vignaraja, Ayla Claire Newton, Robbie Ray, Peter Lam
{"title":"微创拇外翻手术后第一跖骨截骨愈合的初步影像学分型。","authors":"Thomas L Lewis, Sanjana Mehrotra, Jonathan Kaplan, Tyler Gonzalez, Sergio Morales, Thomas J Goff, Vikramman Vignaraja, Ayla Claire Newton, Robbie Ray, Peter Lam","doi":"10.1177/24730114251345818","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Minimally invasive or percutaneous surgery (MIS) for hallux valgus correction has seen increased adoption because of a growing evidence base of positive clinical and radiographic outcomes following surgery. However, no standardized or validated radiographic classification exists to evaluate the first metatarsal osteotomy healing following MIS hallux valgus surgery. The aim was to develop a new radiographic classification system for assessing bone healing following MIS distal transverse osteotomy for hallux valgus.</p><p><strong>Methods: </strong>A 4-domain radiographic classification system based on callus formation, anteroposterior (AP) osteotomy line, lateral osteotomy line, and remodeling for MIS osteotomy healing was developed and tested on a cohort of 27 feet that underwent percutaneous transverse osteotomy for hallux valgus correction. Patients had simultaneous postoperative weightbearing computed tomography (WBCT) and standard radiographs following surgery. Five surgeons reviewed anonymized radiographs to evaluate interobserver reliability. WBCT was used to confirm union status and classification interpretation.</p><p><strong>Results: </strong>The classification system demonstrated substantial interobserver reliability for lateral osteotomy line (Fleiss kappa = 0.671, 95% CI 0.505-0.814) and AP osteotomy line assessment (Fleiss kappa = 0.664, 95% CI 0.459-0.811), with moderate agreement for callus formation (κ = 0.465) and remodeling (κ = 0.439). The classification showed strong correlation with WBCT findings, with an optimal threshold of 8 points identified to differentiate union from nonunion, achieving an overall classification accuracy of 85.2%. This finding was supported by the area under the receiver operating characteristic (ROC) curve of 0.832. At the optimal threshold, the classification demonstrated 90.0% sensitivity and 71.4% specificity for detecting union.</p><p><strong>Conclusion: </strong>This preliminary classification provides a reliable tool for assessing first metatarsal bone healing following MIS hallux valgus osteotomies, with substantial interobserver reliability. It offers a standardized approach for radiographic evaluation, which may enhance comparability across studies and serve as a radiographic research tool pending further validation. Its clinical applicability remains to be determined.</p><p><strong>Level of evidence: </strong>Level III, diagnostic study.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 2","pages":"24730114251345818"},"PeriodicalIF":0.0000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214334/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preliminary Radiographic Classification of First Metatarsal Osteotomy Healing Following Minimally Invasive Hallux Valgus Surgery.\",\"authors\":\"Thomas L Lewis, Sanjana Mehrotra, Jonathan Kaplan, Tyler Gonzalez, Sergio Morales, Thomas J Goff, Vikramman Vignaraja, Ayla Claire Newton, Robbie Ray, Peter Lam\",\"doi\":\"10.1177/24730114251345818\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Minimally invasive or percutaneous surgery (MIS) for hallux valgus correction has seen increased adoption because of a growing evidence base of positive clinical and radiographic outcomes following surgery. However, no standardized or validated radiographic classification exists to evaluate the first metatarsal osteotomy healing following MIS hallux valgus surgery. The aim was to develop a new radiographic classification system for assessing bone healing following MIS distal transverse osteotomy for hallux valgus.</p><p><strong>Methods: </strong>A 4-domain radiographic classification system based on callus formation, anteroposterior (AP) osteotomy line, lateral osteotomy line, and remodeling for MIS osteotomy healing was developed and tested on a cohort of 27 feet that underwent percutaneous transverse osteotomy for hallux valgus correction. Patients had simultaneous postoperative weightbearing computed tomography (WBCT) and standard radiographs following surgery. Five surgeons reviewed anonymized radiographs to evaluate interobserver reliability. WBCT was used to confirm union status and classification interpretation.</p><p><strong>Results: </strong>The classification system demonstrated substantial interobserver reliability for lateral osteotomy line (Fleiss kappa = 0.671, 95% CI 0.505-0.814) and AP osteotomy line assessment (Fleiss kappa = 0.664, 95% CI 0.459-0.811), with moderate agreement for callus formation (κ = 0.465) and remodeling (κ = 0.439). The classification showed strong correlation with WBCT findings, with an optimal threshold of 8 points identified to differentiate union from nonunion, achieving an overall classification accuracy of 85.2%. This finding was supported by the area under the receiver operating characteristic (ROC) curve of 0.832. At the optimal threshold, the classification demonstrated 90.0% sensitivity and 71.4% specificity for detecting union.</p><p><strong>Conclusion: </strong>This preliminary classification provides a reliable tool for assessing first metatarsal bone healing following MIS hallux valgus osteotomies, with substantial interobserver reliability. It offers a standardized approach for radiographic evaluation, which may enhance comparability across studies and serve as a radiographic research tool pending further validation. Its clinical applicability remains to be determined.</p><p><strong>Level of evidence: </strong>Level III, diagnostic study.</p>\",\"PeriodicalId\":12429,\"journal\":{\"name\":\"Foot & Ankle Orthopaedics\",\"volume\":\"10 2\",\"pages\":\"24730114251345818\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214334/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Foot & Ankle Orthopaedics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/24730114251345818\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251345818","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:微创或经皮手术(MIS)矫正拇外翻已被越来越多的采用,因为越来越多的证据表明,手术后的临床和影像学结果是积极的。然而,目前尚无标准化或有效的影像学分类来评估MIS拇外翻手术后首次跖骨截骨愈合情况。目的是开发一种新的影像学分类系统,用于评估拇外翻远端横截骨术后骨愈合情况。方法:基于骨痂形成、前后(AP)截骨线、外侧截骨线和MIS截骨愈合重建的四域放射学分类系统被开发出来,并在27英尺接受经皮横截骨术矫正拇外翻的队列中进行了测试。术后患者同时进行负重计算机断层扫描(WBCT)和标准x线片检查。五名外科医生回顾了匿名的x线照片,以评估观察者之间的可靠性。WBCT用于确定连系状态和分类解释。结果:该分类系统在侧截骨线评估(Fleiss kappa = 0.671, 95% CI 0.505-0.814)和正侧截骨线评估(Fleiss kappa = 0.664, 95% CI 0.459-0.811)方面具有较高的可信度,在骨痂形成(κ = 0.465)和骨重塑(κ = 0.439)方面具有中等程度的一致性。该分类与WBCT结果有很强的相关性,确定了8点的最佳阈值来区分愈合和不愈合,总体分类准确率为85.2%。受试者工作特征(ROC)曲线下面积为0.832,证实了这一结论。在最佳阈值下,该分类对结合体的检测灵敏度为90.0%,特异性为71.4%。结论:该初步分类为评估MIS拇外翻截骨术后第一跖骨愈合提供了可靠的工具,具有较高的观察者间可靠性。它为放射学评估提供了一种标准化的方法,可以增强研究之间的可比性,并作为放射学研究工具等待进一步验证。其临床适用性仍有待确定。证据等级:III级,诊断性研究。
Preliminary Radiographic Classification of First Metatarsal Osteotomy Healing Following Minimally Invasive Hallux Valgus Surgery.
Background: Minimally invasive or percutaneous surgery (MIS) for hallux valgus correction has seen increased adoption because of a growing evidence base of positive clinical and radiographic outcomes following surgery. However, no standardized or validated radiographic classification exists to evaluate the first metatarsal osteotomy healing following MIS hallux valgus surgery. The aim was to develop a new radiographic classification system for assessing bone healing following MIS distal transverse osteotomy for hallux valgus.
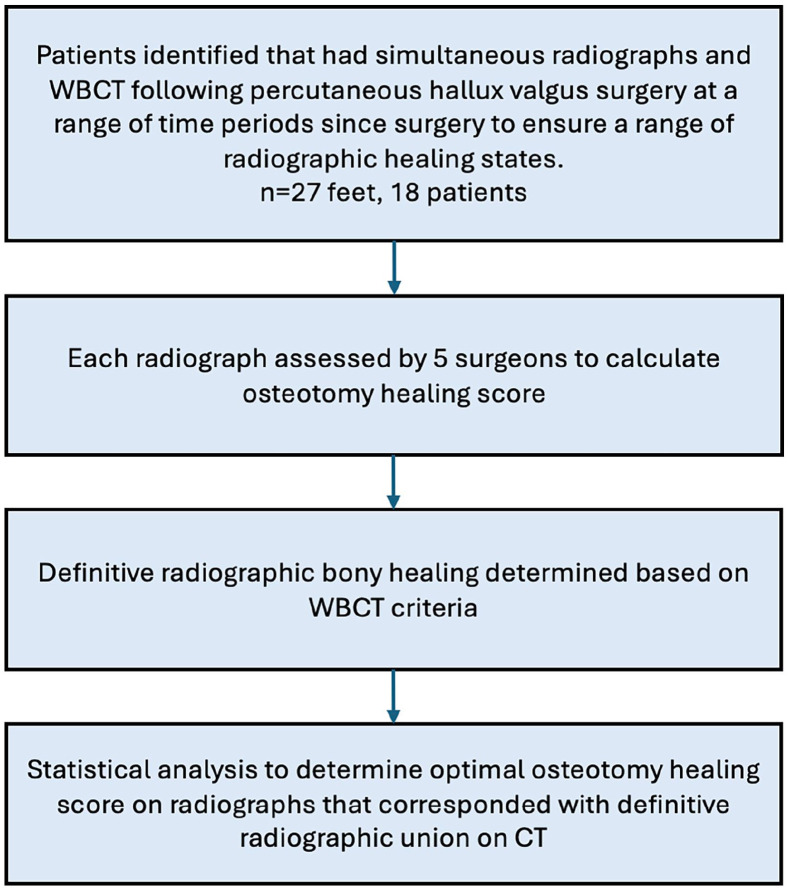
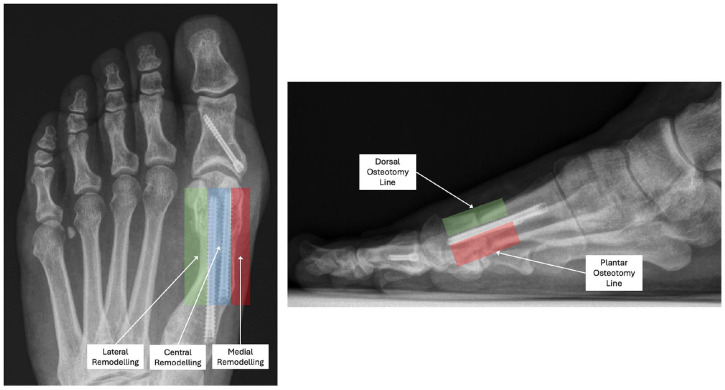
Methods: A 4-domain radiographic classification system based on callus formation, anteroposterior (AP) osteotomy line, lateral osteotomy line, and remodeling for MIS osteotomy healing was developed and tested on a cohort of 27 feet that underwent percutaneous transverse osteotomy for hallux valgus correction. Patients had simultaneous postoperative weightbearing computed tomography (WBCT) and standard radiographs following surgery. Five surgeons reviewed anonymized radiographs to evaluate interobserver reliability. WBCT was used to confirm union status and classification interpretation.
Results: The classification system demonstrated substantial interobserver reliability for lateral osteotomy line (Fleiss kappa = 0.671, 95% CI 0.505-0.814) and AP osteotomy line assessment (Fleiss kappa = 0.664, 95% CI 0.459-0.811), with moderate agreement for callus formation (κ = 0.465) and remodeling (κ = 0.439). The classification showed strong correlation with WBCT findings, with an optimal threshold of 8 points identified to differentiate union from nonunion, achieving an overall classification accuracy of 85.2%. This finding was supported by the area under the receiver operating characteristic (ROC) curve of 0.832. At the optimal threshold, the classification demonstrated 90.0% sensitivity and 71.4% specificity for detecting union.
Conclusion: This preliminary classification provides a reliable tool for assessing first metatarsal bone healing following MIS hallux valgus osteotomies, with substantial interobserver reliability. It offers a standardized approach for radiographic evaluation, which may enhance comparability across studies and serve as a radiographic research tool pending further validation. Its clinical applicability remains to be determined.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


