Christie Rampersad, Aaron Trachtenberg, James Shaw, Nancy Dodd, Krista Maxwell, Martin Karpinski, Chris Wiebe, Peter Nickerson, Julie Ho
{"title":"项目报告-马尼托巴成人肾脏移植项目削减成本,而不是投机取角:质量改进倡议的价值。","authors":"Christie Rampersad, Aaron Trachtenberg, James Shaw, Nancy Dodd, Krista Maxwell, Martin Karpinski, Chris Wiebe, Peter Nickerson, Julie Ho","doi":"10.1177/20543581251341712","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Provision of high-quality, evidence-based patient care that is sustainable for our universal health system is a core Canadian Medical Education Directions for Specialists (CanMEDs) expectation. The Transplant Manitoba Adult Kidney Program (TMAKP) embraced this responsibility by addressing inefficiencies in its practices through multipronged quality improvement (QI) strategies, including reducing unnecessary interventions, implementing innovative strategies, and aligning clinical practices with emerging evidence. Using seamlessly embedded continuous QI and clinical research with a learning health system, the program achieved substantial cost savings and increased opportunities for deceased donor kidney transplantation. The purpose of this analysis is to measure the cost savings associated with these QI initiatives.</p><p><strong>Sources of information: </strong>Transplant Manitoba Adult Kidney Program database and quality metrics, Manitoba Health Physician's Manual (April 1, 2024), PubMed.</p><p><strong>Methods: </strong>To quantify the potential cost savings, we employed a 3-pronged approach. For reduced testing, a cost-counting exercise was conducted using historical transplant activity (831 prevalent and 83 incident patients) to project number of tests avoided and direct costs per test. Second, cost savings for generic mycophenolic acid was presented as ratios of generic to brand name drug costs, and projected cost savings for prevalent patients receiving average dosing. Third, for increased kidney utilization, cost savings per kidney transplant were derived from published studies and extrapolated using predicted additional transplants. Net health care system savings across payers were assessed at a 1-year time horizon.</p><p><strong>Key findings: </strong>The TMAKP reduced unnecessary testing, adopted generic medications, and implemented innovative strategies, achieving $2,530,026 in projected annual 1-year cost savings. These QI initiative savings augment the overall cost-effectiveness of kidney transplantation compared with dialysis. Implementing evidence-based protocols using personalized risk-stratified approaches to viral monitoring and novel donor-specific antibody surveillance strategies aligned testing with clinical risk while minimizing patient burden, highlighting the benefits of seamlessly integrating research with learning health systems. Programs for hepatitis C-viremic donor kidneys and age-targeted allocation increased transplant opportunities and optimized deceased donor organ use. Manitoba's initiatives demonstrate the importance of validation, stakeholder engagement, and iterative adaptation in driving sustainable improvements in transplantation care. Critically, this requires the foresight of health care administrative systems to invest in effective and ongoing QI and embed research with clinical practice, to improve patient and health system outcomes.</p><p><strong>Limitations: </strong>This analysis is limited by reliance on projected cost savings, which require validation through real-world audits to confirm impact. In addition, some valuable QI efforts, while improving patient outcomes, may increase costs, highlighting the need for balanced perspectives in assessing stewardship initiatives. Finally, this analysis is limited to projected cost savings and does not evaluate clinical outcomes, process adherence, or implementation effectiveness.</p><p><strong>Implications: </strong>This experience highlights the potential for QI initiatives to optimize care and resource utilization within Canada's publicly funded health system. These efforts reduced unnecessary testing, minimized patient burden, and expanded transplant opportunities, illustrating how stewardship can balance fiscal responsibility with high-quality state-of-the-art patient care. By implementing evidence-based protocols, TMAKP achieved an additional $2,530,026 in projected cost savings at 1 year. Future annual cost savings will continue rising in a growing prevalent kidney transplant population in Manitoba. These savings can be reallocated to other critical health care services, expanding access and improving outcomes for patients beyond transplantation.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251341712"},"PeriodicalIF":1.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12217574/pdf/","citationCount":"0","resultStr":"{\"title\":\"Program Report-Transplant Manitoba Adult Kidney Program Cutting Costs, Not Corners: Value of Quality Improvement Initiatives.\",\"authors\":\"Christie Rampersad, Aaron Trachtenberg, James Shaw, Nancy Dodd, Krista Maxwell, Martin Karpinski, Chris Wiebe, Peter Nickerson, Julie Ho\",\"doi\":\"10.1177/20543581251341712\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Provision of high-quality, evidence-based patient care that is sustainable for our universal health system is a core Canadian Medical Education Directions for Specialists (CanMEDs) expectation. The Transplant Manitoba Adult Kidney Program (TMAKP) embraced this responsibility by addressing inefficiencies in its practices through multipronged quality improvement (QI) strategies, including reducing unnecessary interventions, implementing innovative strategies, and aligning clinical practices with emerging evidence. Using seamlessly embedded continuous QI and clinical research with a learning health system, the program achieved substantial cost savings and increased opportunities for deceased donor kidney transplantation. The purpose of this analysis is to measure the cost savings associated with these QI initiatives.</p><p><strong>Sources of information: </strong>Transplant Manitoba Adult Kidney Program database and quality metrics, Manitoba Health Physician's Manual (April 1, 2024), PubMed.</p><p><strong>Methods: </strong>To quantify the potential cost savings, we employed a 3-pronged approach. For reduced testing, a cost-counting exercise was conducted using historical transplant activity (831 prevalent and 83 incident patients) to project number of tests avoided and direct costs per test. Second, cost savings for generic mycophenolic acid was presented as ratios of generic to brand name drug costs, and projected cost savings for prevalent patients receiving average dosing. Third, for increased kidney utilization, cost savings per kidney transplant were derived from published studies and extrapolated using predicted additional transplants. Net health care system savings across payers were assessed at a 1-year time horizon.</p><p><strong>Key findings: </strong>The TMAKP reduced unnecessary testing, adopted generic medications, and implemented innovative strategies, achieving $2,530,026 in projected annual 1-year cost savings. These QI initiative savings augment the overall cost-effectiveness of kidney transplantation compared with dialysis. Implementing evidence-based protocols using personalized risk-stratified approaches to viral monitoring and novel donor-specific antibody surveillance strategies aligned testing with clinical risk while minimizing patient burden, highlighting the benefits of seamlessly integrating research with learning health systems. Programs for hepatitis C-viremic donor kidneys and age-targeted allocation increased transplant opportunities and optimized deceased donor organ use. Manitoba's initiatives demonstrate the importance of validation, stakeholder engagement, and iterative adaptation in driving sustainable improvements in transplantation care. Critically, this requires the foresight of health care administrative systems to invest in effective and ongoing QI and embed research with clinical practice, to improve patient and health system outcomes.</p><p><strong>Limitations: </strong>This analysis is limited by reliance on projected cost savings, which require validation through real-world audits to confirm impact. In addition, some valuable QI efforts, while improving patient outcomes, may increase costs, highlighting the need for balanced perspectives in assessing stewardship initiatives. Finally, this analysis is limited to projected cost savings and does not evaluate clinical outcomes, process adherence, or implementation effectiveness.</p><p><strong>Implications: </strong>This experience highlights the potential for QI initiatives to optimize care and resource utilization within Canada's publicly funded health system. These efforts reduced unnecessary testing, minimized patient burden, and expanded transplant opportunities, illustrating how stewardship can balance fiscal responsibility with high-quality state-of-the-art patient care. By implementing evidence-based protocols, TMAKP achieved an additional $2,530,026 in projected cost savings at 1 year. Future annual cost savings will continue rising in a growing prevalent kidney transplant population in Manitoba. These savings can be reallocated to other critical health care services, expanding access and improving outcomes for patients beyond transplantation.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"12 \",\"pages\":\"20543581251341712\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12217574/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581251341712\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251341712","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Program Report-Transplant Manitoba Adult Kidney Program Cutting Costs, Not Corners: Value of Quality Improvement Initiatives.
Purpose: Provision of high-quality, evidence-based patient care that is sustainable for our universal health system is a core Canadian Medical Education Directions for Specialists (CanMEDs) expectation. The Transplant Manitoba Adult Kidney Program (TMAKP) embraced this responsibility by addressing inefficiencies in its practices through multipronged quality improvement (QI) strategies, including reducing unnecessary interventions, implementing innovative strategies, and aligning clinical practices with emerging evidence. Using seamlessly embedded continuous QI and clinical research with a learning health system, the program achieved substantial cost savings and increased opportunities for deceased donor kidney transplantation. The purpose of this analysis is to measure the cost savings associated with these QI initiatives.
Sources of information: Transplant Manitoba Adult Kidney Program database and quality metrics, Manitoba Health Physician's Manual (April 1, 2024), PubMed.
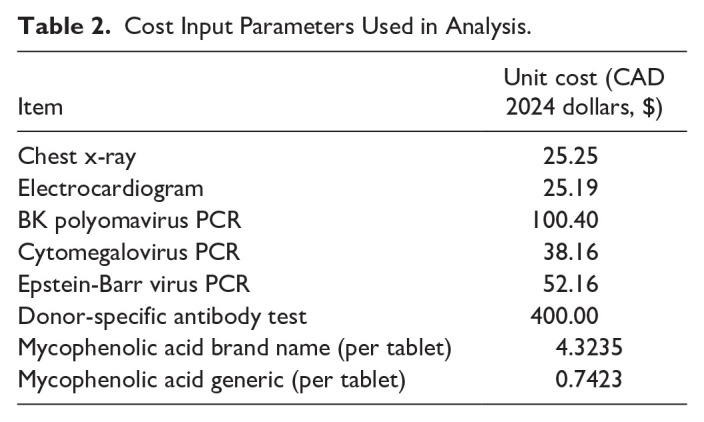
Methods: To quantify the potential cost savings, we employed a 3-pronged approach. For reduced testing, a cost-counting exercise was conducted using historical transplant activity (831 prevalent and 83 incident patients) to project number of tests avoided and direct costs per test. Second, cost savings for generic mycophenolic acid was presented as ratios of generic to brand name drug costs, and projected cost savings for prevalent patients receiving average dosing. Third, for increased kidney utilization, cost savings per kidney transplant were derived from published studies and extrapolated using predicted additional transplants. Net health care system savings across payers were assessed at a 1-year time horizon.
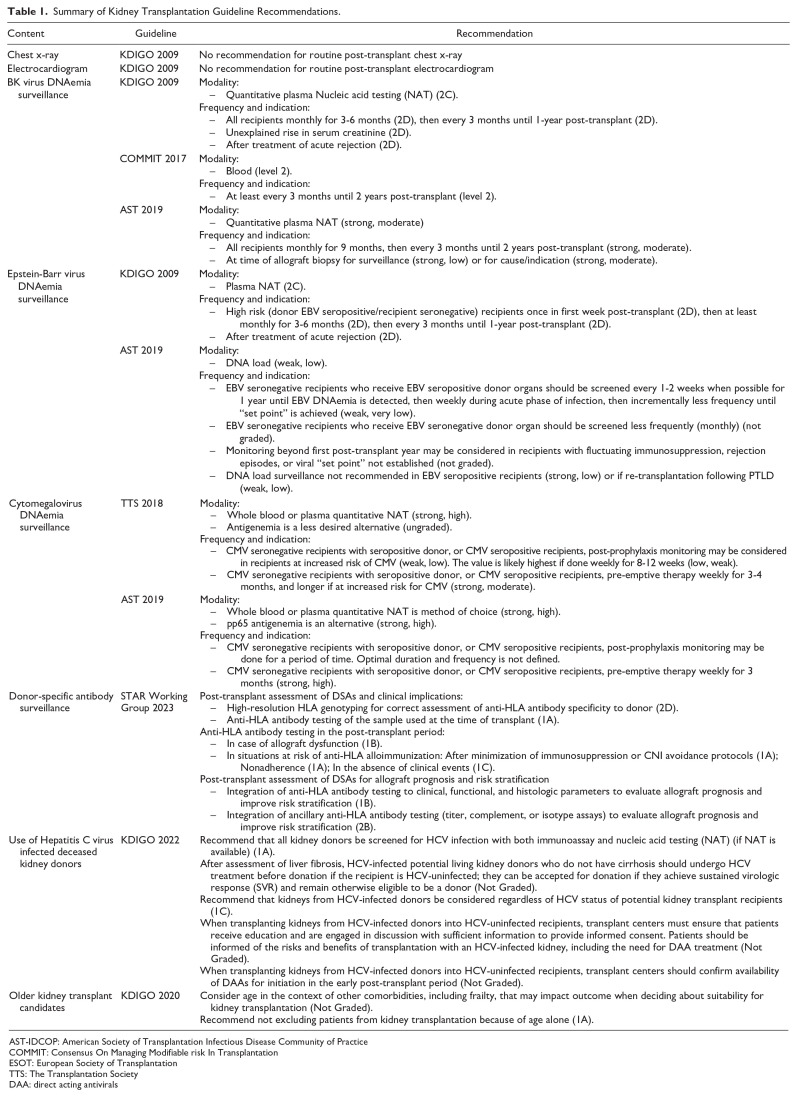
Key findings: The TMAKP reduced unnecessary testing, adopted generic medications, and implemented innovative strategies, achieving $2,530,026 in projected annual 1-year cost savings. These QI initiative savings augment the overall cost-effectiveness of kidney transplantation compared with dialysis. Implementing evidence-based protocols using personalized risk-stratified approaches to viral monitoring and novel donor-specific antibody surveillance strategies aligned testing with clinical risk while minimizing patient burden, highlighting the benefits of seamlessly integrating research with learning health systems. Programs for hepatitis C-viremic donor kidneys and age-targeted allocation increased transplant opportunities and optimized deceased donor organ use. Manitoba's initiatives demonstrate the importance of validation, stakeholder engagement, and iterative adaptation in driving sustainable improvements in transplantation care. Critically, this requires the foresight of health care administrative systems to invest in effective and ongoing QI and embed research with clinical practice, to improve patient and health system outcomes.
Limitations: This analysis is limited by reliance on projected cost savings, which require validation through real-world audits to confirm impact. In addition, some valuable QI efforts, while improving patient outcomes, may increase costs, highlighting the need for balanced perspectives in assessing stewardship initiatives. Finally, this analysis is limited to projected cost savings and does not evaluate clinical outcomes, process adherence, or implementation effectiveness.
Implications: This experience highlights the potential for QI initiatives to optimize care and resource utilization within Canada's publicly funded health system. These efforts reduced unnecessary testing, minimized patient burden, and expanded transplant opportunities, illustrating how stewardship can balance fiscal responsibility with high-quality state-of-the-art patient care. By implementing evidence-based protocols, TMAKP achieved an additional $2,530,026 in projected cost savings at 1 year. Future annual cost savings will continue rising in a growing prevalent kidney transplant population in Manitoba. These savings can be reallocated to other critical health care services, expanding access and improving outcomes for patients beyond transplantation.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


