Tran Nguyen Phuong Hai, Nguyen Nhat Tai, Nguyen Minh Kha, Ly Quang Sang, Pham Thanh Truong Son, Ngo Minh Hung, Le Trung Nhan, Truong The Hiep, Hoang Van Sy
{"title":"重新评估越南心血管风险分层:来自SCORE2和原始SCORE模型的见解","authors":"Tran Nguyen Phuong Hai, Nguyen Nhat Tai, Nguyen Minh Kha, Ly Quang Sang, Pham Thanh Truong Son, Ngo Minh Hung, Le Trung Nhan, Truong The Hiep, Hoang Van Sy","doi":"10.5455/aim.2025.33.112-117","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular disease (CVD) remains a leading cause of morbidity and mortality worldwide, especially in low- and middle-income countries like Vietnam. Risk stratification models such as the original SCORE model have been widely used to guide preventive strategies. Recently, the updated SCORE2 model has been developed to enhance prediction accuracy by incorporating non-fatal events and recalibration for different European regions.</p><p><strong>Objective: </strong>This study aims to compare the performance and applicability of SCORE2 versus the original SCORE in a Vietnamese population undergoing general health check-ups.</p><p><strong>Methods: </strong>We conducted a cross-sectional study on individuals attending general health check-ups at Cho Ray Hospital, a leading tertiary hospital in Vietnam, from January 2024 to July 2024. Demographic, clinical, and laboratory data were collected to calculate cardiovascular risk scores using both the original SCORE and the updated SCORE2 models.</p><p><strong>Results: </strong>Among 477 individuals undergoing general health check-ups, 317 patients met the inclusion criteria with a median age of 54.5 years (IQR: 47-62) and 35% were male. Risk stratification using the original SCORE model classified 87.1% as low-to-moderate risk, 9.1% as high risk, and 3.8% as very high risk. In contrast, SCORE2 reclassified 48.6% as low-to-moderate risk, while high and very high-risk categories increased to 35.6% and 15.8%, respectively (p < 0.001). Notably, 122 out of 276 patients (44.2%) initially classified as low-to-moderate risk by SCORE were reclassified by SCORE2 into higher risk categories - 101 (high risk) and 21 (very high risk). Similarly, 58.6% (n = 17) of patients classified as high risk by SCORE were upgraded to very high risk by SCORE2. SCORE2 also identified more high and very high-risk individuals under 50 years old, particularly among male patients.</p><p><strong>Conclusion: </strong>Compared to the original SCORE model, SCORE2 significantly increased the detection of high and very high cardiovascular risk in Vietnamese individuals undergoing routine health check-ups. The findings suggest that SCORE2 may provide improved risk stratification, especially in younger and male populations, and may better support preventive cardiovascular strategies in clinical practice.</p>","PeriodicalId":7074,"journal":{"name":"Acta Informatica Medica","volume":"33 2","pages":"112-117"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212282/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reassessing Cardiovascular Risk Stratification in Vietnam: Insights from SCORE2 and the Original SCORE Model.\",\"authors\":\"Tran Nguyen Phuong Hai, Nguyen Nhat Tai, Nguyen Minh Kha, Ly Quang Sang, Pham Thanh Truong Son, Ngo Minh Hung, Le Trung Nhan, Truong The Hiep, Hoang Van Sy\",\"doi\":\"10.5455/aim.2025.33.112-117\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiovascular disease (CVD) remains a leading cause of morbidity and mortality worldwide, especially in low- and middle-income countries like Vietnam. Risk stratification models such as the original SCORE model have been widely used to guide preventive strategies. Recently, the updated SCORE2 model has been developed to enhance prediction accuracy by incorporating non-fatal events and recalibration for different European regions.</p><p><strong>Objective: </strong>This study aims to compare the performance and applicability of SCORE2 versus the original SCORE in a Vietnamese population undergoing general health check-ups.</p><p><strong>Methods: </strong>We conducted a cross-sectional study on individuals attending general health check-ups at Cho Ray Hospital, a leading tertiary hospital in Vietnam, from January 2024 to July 2024. Demographic, clinical, and laboratory data were collected to calculate cardiovascular risk scores using both the original SCORE and the updated SCORE2 models.</p><p><strong>Results: </strong>Among 477 individuals undergoing general health check-ups, 317 patients met the inclusion criteria with a median age of 54.5 years (IQR: 47-62) and 35% were male. Risk stratification using the original SCORE model classified 87.1% as low-to-moderate risk, 9.1% as high risk, and 3.8% as very high risk. In contrast, SCORE2 reclassified 48.6% as low-to-moderate risk, while high and very high-risk categories increased to 35.6% and 15.8%, respectively (p < 0.001). Notably, 122 out of 276 patients (44.2%) initially classified as low-to-moderate risk by SCORE were reclassified by SCORE2 into higher risk categories - 101 (high risk) and 21 (very high risk). Similarly, 58.6% (n = 17) of patients classified as high risk by SCORE were upgraded to very high risk by SCORE2. SCORE2 also identified more high and very high-risk individuals under 50 years old, particularly among male patients.</p><p><strong>Conclusion: </strong>Compared to the original SCORE model, SCORE2 significantly increased the detection of high and very high cardiovascular risk in Vietnamese individuals undergoing routine health check-ups. The findings suggest that SCORE2 may provide improved risk stratification, especially in younger and male populations, and may better support preventive cardiovascular strategies in clinical practice.</p>\",\"PeriodicalId\":7074,\"journal\":{\"name\":\"Acta Informatica Medica\",\"volume\":\"33 2\",\"pages\":\"112-117\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12212282/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta Informatica Medica\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5455/aim.2025.33.112-117\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Informatica Medica","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5455/aim.2025.33.112-117","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Reassessing Cardiovascular Risk Stratification in Vietnam: Insights from SCORE2 and the Original SCORE Model.
Background: Cardiovascular disease (CVD) remains a leading cause of morbidity and mortality worldwide, especially in low- and middle-income countries like Vietnam. Risk stratification models such as the original SCORE model have been widely used to guide preventive strategies. Recently, the updated SCORE2 model has been developed to enhance prediction accuracy by incorporating non-fatal events and recalibration for different European regions.
Objective: This study aims to compare the performance and applicability of SCORE2 versus the original SCORE in a Vietnamese population undergoing general health check-ups.
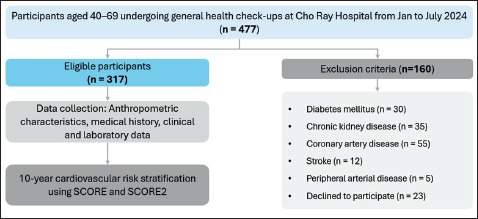
Methods: We conducted a cross-sectional study on individuals attending general health check-ups at Cho Ray Hospital, a leading tertiary hospital in Vietnam, from January 2024 to July 2024. Demographic, clinical, and laboratory data were collected to calculate cardiovascular risk scores using both the original SCORE and the updated SCORE2 models.
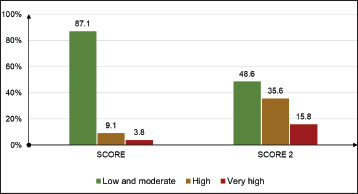
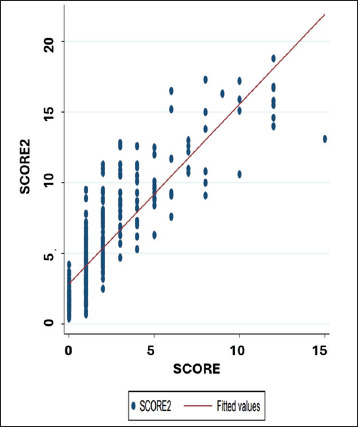
Results: Among 477 individuals undergoing general health check-ups, 317 patients met the inclusion criteria with a median age of 54.5 years (IQR: 47-62) and 35% were male. Risk stratification using the original SCORE model classified 87.1% as low-to-moderate risk, 9.1% as high risk, and 3.8% as very high risk. In contrast, SCORE2 reclassified 48.6% as low-to-moderate risk, while high and very high-risk categories increased to 35.6% and 15.8%, respectively (p < 0.001). Notably, 122 out of 276 patients (44.2%) initially classified as low-to-moderate risk by SCORE were reclassified by SCORE2 into higher risk categories - 101 (high risk) and 21 (very high risk). Similarly, 58.6% (n = 17) of patients classified as high risk by SCORE were upgraded to very high risk by SCORE2. SCORE2 also identified more high and very high-risk individuals under 50 years old, particularly among male patients.
Conclusion: Compared to the original SCORE model, SCORE2 significantly increased the detection of high and very high cardiovascular risk in Vietnamese individuals undergoing routine health check-ups. The findings suggest that SCORE2 may provide improved risk stratification, especially in younger and male populations, and may better support preventive cardiovascular strategies in clinical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


