{"title":"弥漫性大b细胞淋巴瘤患者中枢神经系统复发的基因组危险因素。","authors":"Shiyu Jiang, Qunling Zhang, Jia Jin, Wenhao Zhang","doi":"10.1007/s44313-025-00087-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Central nervous system (CNS) relapse is associated with poor survival, and remains an unmet challenge in patients with diffuse large B-cell lymphoma (DLBCL). Identifying patients at high risk of CNS relapse and offering prophylactic treatment could improve patient prognosis.</p><p><strong>Methods: </strong>Here, we studied 234 patients with DLBCL using open patient-level clinical and sequencing data to explore risk factors for CNS relapse. Patients were divided into Cohort A (CNS involvement at baseline), Cohort B (CNS recurrence), and Cohort C (patients without secondary CNS involvement and with a follow-up interval > 3 years). We investigated the risk factors for CNS relapse in Cohorts B + C.</p><p><strong>Results: </strong>Genetic alterations with statistical significance, determined by univariate analysis, and an incidence rate ≥ 5%, together with clinical factors, correlated with CNS relapse risk in a multivariate analysis. Multivariate logistic regression analysis revealed that concomitant MYD88 L265P and CDKN2A loss (p = 0.012), TET2 mutation (p = 0.037), ARID1A mutation (p = 0.010), and INO80 (p = 0.002) were independently correlated with a high risk of CNS relapse after adjusting for the IPI risk groups, B symptom and cell of origin (COO). The classifier that integrated genomic risk factors was superior in predicting CNS relapse (area under the receiver operating characteristic curve [AUROC]: 0.91) compared with the IPI (AUROC: 0.77, p < 0.001) or IPI in combination with COO classifiers (AUROC: 0.81, p = 0.013).</p><p><strong>Conclusion: </strong>This study identified several genomic alterations as risk factors for CNS relapse.</p>","PeriodicalId":46224,"journal":{"name":"Blood Research","volume":"60 1","pages":"36"},"PeriodicalIF":2.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214237/pdf/","citationCount":"0","resultStr":"{\"title\":\"Genomic risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma.\",\"authors\":\"Shiyu Jiang, Qunling Zhang, Jia Jin, Wenhao Zhang\",\"doi\":\"10.1007/s44313-025-00087-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Central nervous system (CNS) relapse is associated with poor survival, and remains an unmet challenge in patients with diffuse large B-cell lymphoma (DLBCL). Identifying patients at high risk of CNS relapse and offering prophylactic treatment could improve patient prognosis.</p><p><strong>Methods: </strong>Here, we studied 234 patients with DLBCL using open patient-level clinical and sequencing data to explore risk factors for CNS relapse. Patients were divided into Cohort A (CNS involvement at baseline), Cohort B (CNS recurrence), and Cohort C (patients without secondary CNS involvement and with a follow-up interval > 3 years). We investigated the risk factors for CNS relapse in Cohorts B + C.</p><p><strong>Results: </strong>Genetic alterations with statistical significance, determined by univariate analysis, and an incidence rate ≥ 5%, together with clinical factors, correlated with CNS relapse risk in a multivariate analysis. Multivariate logistic regression analysis revealed that concomitant MYD88 L265P and CDKN2A loss (p = 0.012), TET2 mutation (p = 0.037), ARID1A mutation (p = 0.010), and INO80 (p = 0.002) were independently correlated with a high risk of CNS relapse after adjusting for the IPI risk groups, B symptom and cell of origin (COO). The classifier that integrated genomic risk factors was superior in predicting CNS relapse (area under the receiver operating characteristic curve [AUROC]: 0.91) compared with the IPI (AUROC: 0.77, p < 0.001) or IPI in combination with COO classifiers (AUROC: 0.81, p = 0.013).</p><p><strong>Conclusion: </strong>This study identified several genomic alterations as risk factors for CNS relapse.</p>\",\"PeriodicalId\":46224,\"journal\":{\"name\":\"Blood Research\",\"volume\":\"60 1\",\"pages\":\"36\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12214237/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Blood Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s44313-025-00087-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s44313-025-00087-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Genomic risk factors for central nervous system relapse in patients with diffuse large B-cell lymphoma.
Purpose: Central nervous system (CNS) relapse is associated with poor survival, and remains an unmet challenge in patients with diffuse large B-cell lymphoma (DLBCL). Identifying patients at high risk of CNS relapse and offering prophylactic treatment could improve patient prognosis.
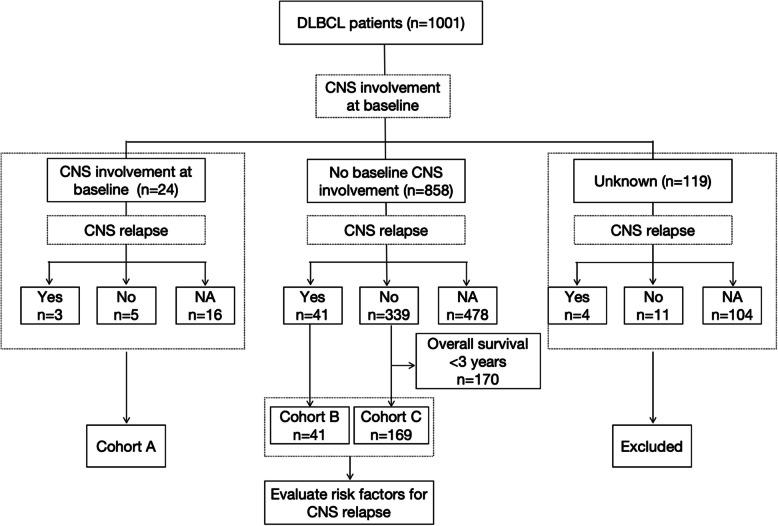
Methods: Here, we studied 234 patients with DLBCL using open patient-level clinical and sequencing data to explore risk factors for CNS relapse. Patients were divided into Cohort A (CNS involvement at baseline), Cohort B (CNS recurrence), and Cohort C (patients without secondary CNS involvement and with a follow-up interval > 3 years). We investigated the risk factors for CNS relapse in Cohorts B + C.
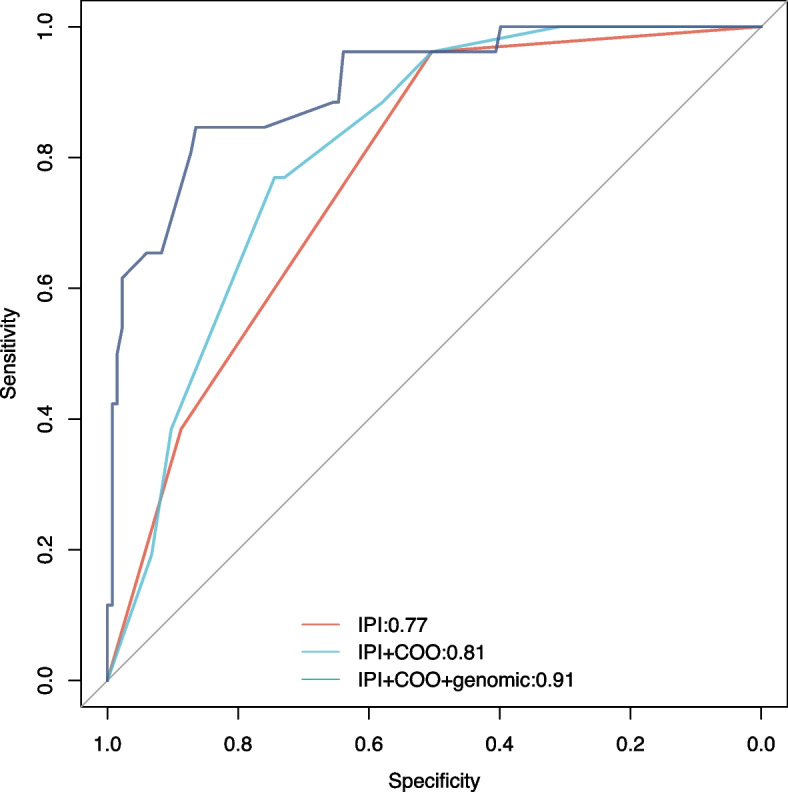
Results: Genetic alterations with statistical significance, determined by univariate analysis, and an incidence rate ≥ 5%, together with clinical factors, correlated with CNS relapse risk in a multivariate analysis. Multivariate logistic regression analysis revealed that concomitant MYD88 L265P and CDKN2A loss (p = 0.012), TET2 mutation (p = 0.037), ARID1A mutation (p = 0.010), and INO80 (p = 0.002) were independently correlated with a high risk of CNS relapse after adjusting for the IPI risk groups, B symptom and cell of origin (COO). The classifier that integrated genomic risk factors was superior in predicting CNS relapse (area under the receiver operating characteristic curve [AUROC]: 0.91) compared with the IPI (AUROC: 0.77, p < 0.001) or IPI in combination with COO classifiers (AUROC: 0.81, p = 0.013).
Conclusion: This study identified several genomic alterations as risk factors for CNS relapse.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


