{"title":"慢性复发性多灶性骨髓炎(CRMO)患者队列的诊断和治疗见解。","authors":"Kosar Asna Ashari, Mahdieh Mousavi, Fatemeh Tahghighi Sharabian, Raheleh Assari, Seyyed Reza Raeeskarami, Vahid Ziaee","doi":"10.1186/s41927-025-00537-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic recurrent multifocal osteomyelitis (CRMO) is a sporadic form of autoinflammatory bone disorders (ABDs) presenting with sterile chronic and/or recurrent and multiple sites of bone involvement. We aimed to describe our 10-year cohort of CRMO patients and analyze the characteristics and treatment approaches.</p><p><strong>Methods: </strong>We retrospectively analyzed the data on patients with bone diseases at Children's Medical Center, Tehran University of Medical Sciences, Iran in the previous 10 years. The criteria for inclusion of patients as CNO/CRMO were mono-, oligo- or multifocal inflammatory bone lesions (osteomyelitis, osteitis, osteosclerosis) by imaging techniques; duration of complaints for > 6 weeks; and onset before 18 years of age.</p><p><strong>Results: </strong>Thirty-nine patients were enrolled. Diagnosis of five patients were found compatible with monogenic ABDs. There were four sites of bone involvement per patient. The most common sites were vertebrae, pelvis, and tibia. Eight patients (23%) had dermatologic manifestations, including three psoriasis cases and one palmar pustulosis. All patients received NSAIDs, and 85% received it as first-line. Treatment was escalated to methotrexate or prednisolone when response was suboptimal. Out of 17 patients primarily treated only with NSAIDs, 47% remitted. In general, 84% of our patients are in remission: 36% without medication and 48% with medication.</p><p><strong>Conclusion: </strong>Our CRMO patients showed an acceptable remission response to the current treatment regimen. Results of bone scintigraphy in suspected CRMO patients should be interpreted cautiously as an adjunct to clinical investigations. Special attention should be paid to extraosseous manifestations in suspected CRMO patients to avoid overlooking monogenic ABDs.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9150,"journal":{"name":"BMC Rheumatology","volume":"9 1","pages":"70"},"PeriodicalIF":2.5000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12218946/pdf/","citationCount":"0","resultStr":"{\"title\":\"Diagnostic and therapeutic insights from a cohort of chronic recurrent multifocal osteomyelitis (CRMO) patients.\",\"authors\":\"Kosar Asna Ashari, Mahdieh Mousavi, Fatemeh Tahghighi Sharabian, Raheleh Assari, Seyyed Reza Raeeskarami, Vahid Ziaee\",\"doi\":\"10.1186/s41927-025-00537-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chronic recurrent multifocal osteomyelitis (CRMO) is a sporadic form of autoinflammatory bone disorders (ABDs) presenting with sterile chronic and/or recurrent and multiple sites of bone involvement. We aimed to describe our 10-year cohort of CRMO patients and analyze the characteristics and treatment approaches.</p><p><strong>Methods: </strong>We retrospectively analyzed the data on patients with bone diseases at Children's Medical Center, Tehran University of Medical Sciences, Iran in the previous 10 years. The criteria for inclusion of patients as CNO/CRMO were mono-, oligo- or multifocal inflammatory bone lesions (osteomyelitis, osteitis, osteosclerosis) by imaging techniques; duration of complaints for > 6 weeks; and onset before 18 years of age.</p><p><strong>Results: </strong>Thirty-nine patients were enrolled. Diagnosis of five patients were found compatible with monogenic ABDs. There were four sites of bone involvement per patient. The most common sites were vertebrae, pelvis, and tibia. Eight patients (23%) had dermatologic manifestations, including three psoriasis cases and one palmar pustulosis. All patients received NSAIDs, and 85% received it as first-line. Treatment was escalated to methotrexate or prednisolone when response was suboptimal. Out of 17 patients primarily treated only with NSAIDs, 47% remitted. In general, 84% of our patients are in remission: 36% without medication and 48% with medication.</p><p><strong>Conclusion: </strong>Our CRMO patients showed an acceptable remission response to the current treatment regimen. Results of bone scintigraphy in suspected CRMO patients should be interpreted cautiously as an adjunct to clinical investigations. Special attention should be paid to extraosseous manifestations in suspected CRMO patients to avoid overlooking monogenic ABDs.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>\",\"PeriodicalId\":9150,\"journal\":{\"name\":\"BMC Rheumatology\",\"volume\":\"9 1\",\"pages\":\"70\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12218946/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Rheumatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41927-025-00537-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Rheumatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41927-025-00537-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Diagnostic and therapeutic insights from a cohort of chronic recurrent multifocal osteomyelitis (CRMO) patients.
Background: Chronic recurrent multifocal osteomyelitis (CRMO) is a sporadic form of autoinflammatory bone disorders (ABDs) presenting with sterile chronic and/or recurrent and multiple sites of bone involvement. We aimed to describe our 10-year cohort of CRMO patients and analyze the characteristics and treatment approaches.
Methods: We retrospectively analyzed the data on patients with bone diseases at Children's Medical Center, Tehran University of Medical Sciences, Iran in the previous 10 years. The criteria for inclusion of patients as CNO/CRMO were mono-, oligo- or multifocal inflammatory bone lesions (osteomyelitis, osteitis, osteosclerosis) by imaging techniques; duration of complaints for > 6 weeks; and onset before 18 years of age.
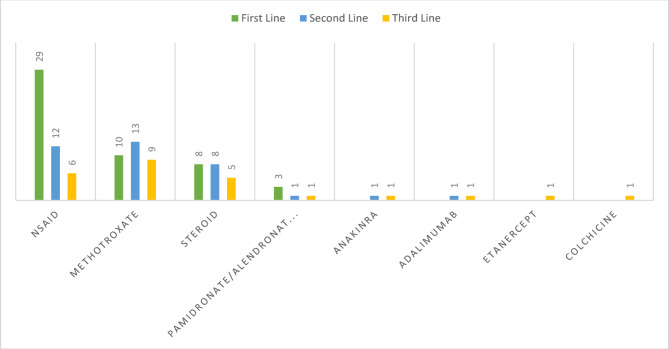
Results: Thirty-nine patients were enrolled. Diagnosis of five patients were found compatible with monogenic ABDs. There were four sites of bone involvement per patient. The most common sites were vertebrae, pelvis, and tibia. Eight patients (23%) had dermatologic manifestations, including three psoriasis cases and one palmar pustulosis. All patients received NSAIDs, and 85% received it as first-line. Treatment was escalated to methotrexate or prednisolone when response was suboptimal. Out of 17 patients primarily treated only with NSAIDs, 47% remitted. In general, 84% of our patients are in remission: 36% without medication and 48% with medication.
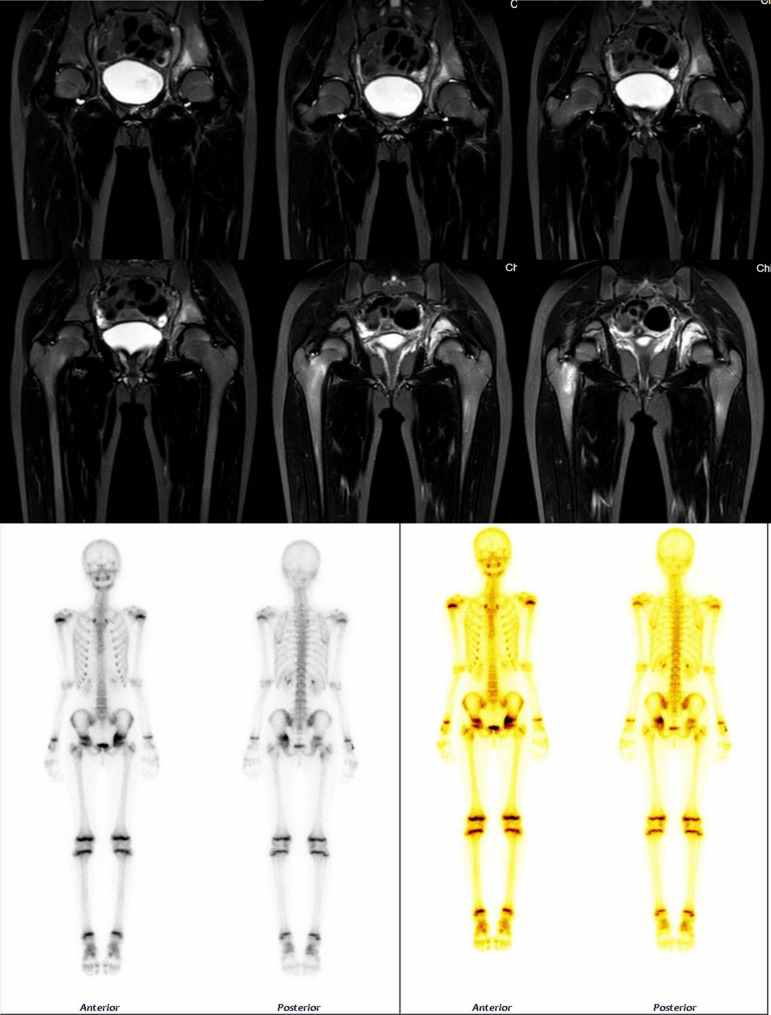
Conclusion: Our CRMO patients showed an acceptable remission response to the current treatment regimen. Results of bone scintigraphy in suspected CRMO patients should be interpreted cautiously as an adjunct to clinical investigations. Special attention should be paid to extraosseous manifestations in suspected CRMO patients to avoid overlooking monogenic ABDs.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


