Amelie Pettrich, Julia Schellong, Anne Dyer, Thomas Ehring, Christine Knaevelsrud, Antje Krüger-Gottschalk, Yuriy Nesterko, Ingo Schäfer, Heide Glaesmer
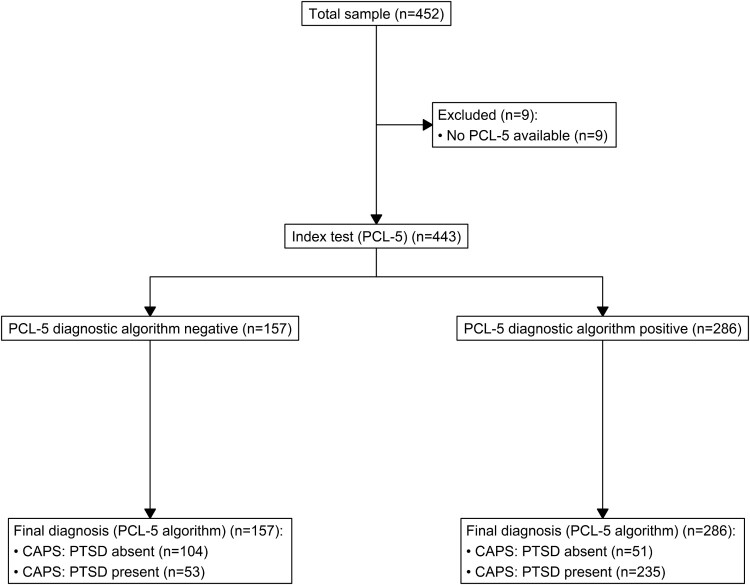
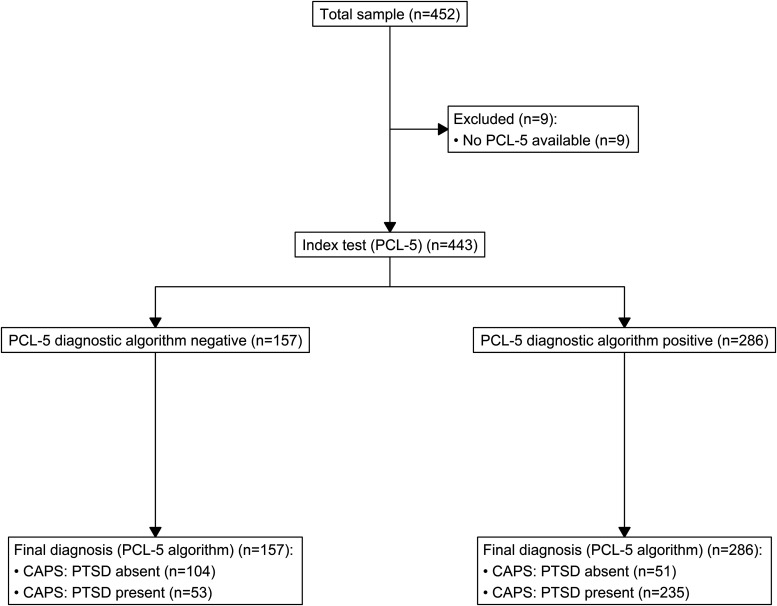
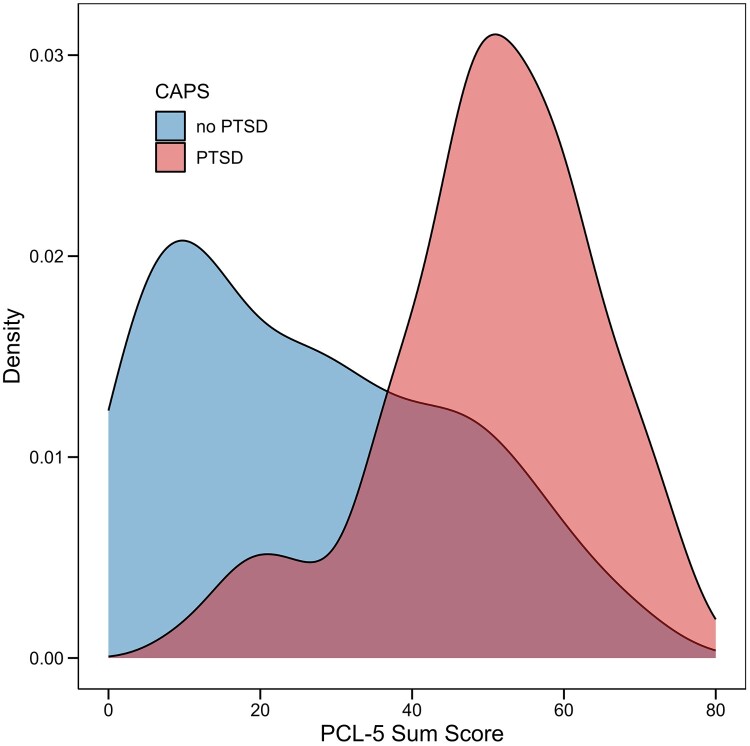
{"title":"超越一个临界值:确定DSM-5 (PCL-5) PTSD检查表的临界值。","authors":"Amelie Pettrich, Julia Schellong, Anne Dyer, Thomas Ehring, Christine Knaevelsrud, Antje Krüger-Gottschalk, Yuriy Nesterko, Ingo Schäfer, Heide Glaesmer","doi":"10.1080/20008066.2025.2514878","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> There is no universally optimal cutoff score for identifying probable PTSD, which makes reliable PTSD diagnosis challenging not only across different populations but also in different settings. Reliable outcomes require tailoring cutoff scores to the population, intended use (clinical, research, or prevalence estimation), and appropriate statistical methods to ensure their validity.<b>Objective:</b> While previously little emphasis has been placed on thorough methodological evaluation and purpose-driven cutoff selection, this work addresses these gaps by evaluating optimal PCL-5 cutoff scores for clinical use, prevalence estimation, and research in a German-speaking clinical sample.<b>Methods:</b> Previously published data from 443 trauma-exposed individuals in Germany were re-analyzed for this purpose. PTSD was assessed using the PCL-5 and with CAPS-5 clinical interview. Optimal cutoffs were identified using ROC analysis, applying standard estimation methods and prioritising diagnostic utility based on specific objectives.<b>Results:</b> After evaluating various cutoff points for different purposes, we identified the following as most suitable for this sample: a cutoff of 34 for clinical use (sensitivity: 0.892, specificity: 0.645, PPV: 0.824, NPV: 0.763); 38 for prevalence estimation (sensitivity: 0.840, specificity: 0.703, PPV: 0.840, NPV: 0.703); and 42 or 43 for identifying clear-cut cases in research or resource-limited settings (sensitivity: 0.774-0.760, specificity: 0.742-0.761, PPV: 0.848-0.855, NPV: 0.639-0.631). The originally intended cutoffs of 31-33 yielded acceptable to excellent diagnostic utility parameters but were not identified as optimal for any specific purpose.<b>Conclusion:</b> This study highlights the variability in optimal PCL-5 cutoffs, linking selection to specific clinical or research aims. It provides validated cutoffs for PTSD prevalence in a German clinical sample, with limitations regarding generalizability to lower-prevalence populations. Future research should refine cutoffs for diverse populations and improve diagnostic precision.</p>","PeriodicalId":12055,"journal":{"name":"European Journal of Psychotraumatology","volume":"16 1","pages":"2514878"},"PeriodicalIF":4.1000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12210402/pdf/","citationCount":"0","resultStr":"{\"title\":\"Beyond one-cutoff-fits-all: determining cutoff values for the PTSD checklist for DSM-5 (PCL-5).\",\"authors\":\"Amelie Pettrich, Julia Schellong, Anne Dyer, Thomas Ehring, Christine Knaevelsrud, Antje Krüger-Gottschalk, Yuriy Nesterko, Ingo Schäfer, Heide Glaesmer\",\"doi\":\"10.1080/20008066.2025.2514878\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> There is no universally optimal cutoff score for identifying probable PTSD, which makes reliable PTSD diagnosis challenging not only across different populations but also in different settings. Reliable outcomes require tailoring cutoff scores to the population, intended use (clinical, research, or prevalence estimation), and appropriate statistical methods to ensure their validity.<b>Objective:</b> While previously little emphasis has been placed on thorough methodological evaluation and purpose-driven cutoff selection, this work addresses these gaps by evaluating optimal PCL-5 cutoff scores for clinical use, prevalence estimation, and research in a German-speaking clinical sample.<b>Methods:</b> Previously published data from 443 trauma-exposed individuals in Germany were re-analyzed for this purpose. PTSD was assessed using the PCL-5 and with CAPS-5 clinical interview. Optimal cutoffs were identified using ROC analysis, applying standard estimation methods and prioritising diagnostic utility based on specific objectives.<b>Results:</b> After evaluating various cutoff points for different purposes, we identified the following as most suitable for this sample: a cutoff of 34 for clinical use (sensitivity: 0.892, specificity: 0.645, PPV: 0.824, NPV: 0.763); 38 for prevalence estimation (sensitivity: 0.840, specificity: 0.703, PPV: 0.840, NPV: 0.703); and 42 or 43 for identifying clear-cut cases in research or resource-limited settings (sensitivity: 0.774-0.760, specificity: 0.742-0.761, PPV: 0.848-0.855, NPV: 0.639-0.631). The originally intended cutoffs of 31-33 yielded acceptable to excellent diagnostic utility parameters but were not identified as optimal for any specific purpose.<b>Conclusion:</b> This study highlights the variability in optimal PCL-5 cutoffs, linking selection to specific clinical or research aims. It provides validated cutoffs for PTSD prevalence in a German clinical sample, with limitations regarding generalizability to lower-prevalence populations. Future research should refine cutoffs for diverse populations and improve diagnostic precision.</p>\",\"PeriodicalId\":12055,\"journal\":{\"name\":\"European Journal of Psychotraumatology\",\"volume\":\"16 1\",\"pages\":\"2514878\"},\"PeriodicalIF\":4.1000,\"publicationDate\":\"2025-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12210402/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Psychotraumatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/20008066.2025.2514878\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Psychotraumatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/20008066.2025.2514878","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/30 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Beyond one-cutoff-fits-all: determining cutoff values for the PTSD checklist for DSM-5 (PCL-5).
Background: There is no universally optimal cutoff score for identifying probable PTSD, which makes reliable PTSD diagnosis challenging not only across different populations but also in different settings. Reliable outcomes require tailoring cutoff scores to the population, intended use (clinical, research, or prevalence estimation), and appropriate statistical methods to ensure their validity.Objective: While previously little emphasis has been placed on thorough methodological evaluation and purpose-driven cutoff selection, this work addresses these gaps by evaluating optimal PCL-5 cutoff scores for clinical use, prevalence estimation, and research in a German-speaking clinical sample.Methods: Previously published data from 443 trauma-exposed individuals in Germany were re-analyzed for this purpose. PTSD was assessed using the PCL-5 and with CAPS-5 clinical interview. Optimal cutoffs were identified using ROC analysis, applying standard estimation methods and prioritising diagnostic utility based on specific objectives.Results: After evaluating various cutoff points for different purposes, we identified the following as most suitable for this sample: a cutoff of 34 for clinical use (sensitivity: 0.892, specificity: 0.645, PPV: 0.824, NPV: 0.763); 38 for prevalence estimation (sensitivity: 0.840, specificity: 0.703, PPV: 0.840, NPV: 0.703); and 42 or 43 for identifying clear-cut cases in research or resource-limited settings (sensitivity: 0.774-0.760, specificity: 0.742-0.761, PPV: 0.848-0.855, NPV: 0.639-0.631). The originally intended cutoffs of 31-33 yielded acceptable to excellent diagnostic utility parameters but were not identified as optimal for any specific purpose.Conclusion: This study highlights the variability in optimal PCL-5 cutoffs, linking selection to specific clinical or research aims. It provides validated cutoffs for PTSD prevalence in a German clinical sample, with limitations regarding generalizability to lower-prevalence populations. Future research should refine cutoffs for diverse populations and improve diagnostic precision.
期刊介绍:
The European Journal of Psychotraumatology (EJPT) is a peer-reviewed open access interdisciplinary journal owned by the European Society of Traumatic Stress Studies (ESTSS). The European Journal of Psychotraumatology (EJPT) aims to engage scholars, clinicians and researchers in the vital issues of how to understand, prevent and treat the consequences of stress and trauma, including but not limited to, posttraumatic stress disorder (PTSD), depressive disorders, substance abuse, burnout, and neurobiological or physical consequences, using the latest research or clinical experience in these areas. The journal shares ESTSS’ mission to advance and disseminate scientific knowledge about traumatic stress. Papers may address individual events, repeated or chronic (complex) trauma, large scale disasters, or violence. Being open access, the European Journal of Psychotraumatology is also evidence of ESTSS’ stand on free accessibility of research publications to a wider community via the web. The European Journal of Psychotraumatology seeks to attract contributions from academics and practitioners from diverse professional backgrounds, including, but not restricted to, those in mental health, social sciences, and health and welfare services. Contributions from outside Europe are welcome. The journal welcomes original basic and clinical research articles that consolidate and expand the theoretical and professional basis of the field of traumatic stress; Review articles including meta-analyses; short communications presenting new ideas or early-stage promising research; study protocols that describe proposed or ongoing research; case reports examining a single individual or event in a real‑life context; clinical practice papers sharing experience from the clinic; letters to the Editor debating articles already published in the Journal; inaugural Lectures; conference abstracts and book reviews. Both quantitative and qualitative research is welcome.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


