Sarjit Singh, Mark Andonovic, Jamie P Traynor, Martin F Shaw, Malcolm A B Sim, Patrick B Mark, Kathryn A Puxty
{"title":"重症监护中少尿和非少尿急性肾损伤的短期和长期结局:一项回顾性、事后、双中心研究。","authors":"Sarjit Singh, Mark Andonovic, Jamie P Traynor, Martin F Shaw, Malcolm A B Sim, Patrick B Mark, Kathryn A Puxty","doi":"10.1093/ckj/sfaf170","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients admitted to intensive care units (ICUs) frequently develop acute kidney injury (AKI). There is limited research comparing outcomes between oliguric and non-oliguric AKI in this population. This study aimed to investigate the short- and long-term outcomes in oliguric and non-oliguric AKI in intensive care patients; the specific outcomes assessed were mortality and major adverse kidney events. We hypothesised that short- and long-term outcomes would be poorer in oliguric compared with non-oliguric AKI in intensive care patients.</p><p><strong>Methods: </strong>This retrospective observational cohort study utilised prospectively collected data routinely gathered during patients' admission. All adult patients >16 years of age admitted to two large Scottish general adult ICUs were included. Patients with long-term kidney replacement therapy, prior transplantation and ICU readmission were excluded. Oliguria was defined as urine output <0.3 ml/kg/h for 24 h. Outcomes were assessed using Cox proportional hazards analyses; should its assumptions be violated, odds ratios at prespecified time points were undertaken.</p><p><strong>Results: </strong>Of the 2147 patients identified with <i>de novo</i> AKI, 1666 had sufficient urine output data for analysis. A total of 528 (31.7%) subjects had oliguric AKI lasting at least 24 h. The 1-year mortality was higher in oliguric patients [adjusted hazard ratio 1.45 (95% confidence interval 1.02-2.12), <i>E</i>-value 1.93]. Our data violated the proportional hazards assumption for major adverse kidney events; the 1-year odds ratio for major adverse renal events was non-significant at 1.25 (95% confidence interval 0.92-1.69).</p><p><strong>Conclusion: </strong>Our study demonstrated that one-third of patients with AKI in intensive care developed oliguria using a standardised definition of oliguria. Oliguric AKI was found to be significantly associated with higher rates of mortality from in-critical care through 1-year post-discharge.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 6","pages":"sfaf170"},"PeriodicalIF":4.6000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12203070/pdf/","citationCount":"0","resultStr":"{\"title\":\"Short- and long-term outcomes in oliguric and non-oliguric acute kidney injury in intensive care: a retrospective, post hoc, bicentric study.\",\"authors\":\"Sarjit Singh, Mark Andonovic, Jamie P Traynor, Martin F Shaw, Malcolm A B Sim, Patrick B Mark, Kathryn A Puxty\",\"doi\":\"10.1093/ckj/sfaf170\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients admitted to intensive care units (ICUs) frequently develop acute kidney injury (AKI). There is limited research comparing outcomes between oliguric and non-oliguric AKI in this population. This study aimed to investigate the short- and long-term outcomes in oliguric and non-oliguric AKI in intensive care patients; the specific outcomes assessed were mortality and major adverse kidney events. We hypothesised that short- and long-term outcomes would be poorer in oliguric compared with non-oliguric AKI in intensive care patients.</p><p><strong>Methods: </strong>This retrospective observational cohort study utilised prospectively collected data routinely gathered during patients' admission. All adult patients >16 years of age admitted to two large Scottish general adult ICUs were included. Patients with long-term kidney replacement therapy, prior transplantation and ICU readmission were excluded. Oliguria was defined as urine output <0.3 ml/kg/h for 24 h. Outcomes were assessed using Cox proportional hazards analyses; should its assumptions be violated, odds ratios at prespecified time points were undertaken.</p><p><strong>Results: </strong>Of the 2147 patients identified with <i>de novo</i> AKI, 1666 had sufficient urine output data for analysis. A total of 528 (31.7%) subjects had oliguric AKI lasting at least 24 h. The 1-year mortality was higher in oliguric patients [adjusted hazard ratio 1.45 (95% confidence interval 1.02-2.12), <i>E</i>-value 1.93]. Our data violated the proportional hazards assumption for major adverse kidney events; the 1-year odds ratio for major adverse renal events was non-significant at 1.25 (95% confidence interval 0.92-1.69).</p><p><strong>Conclusion: </strong>Our study demonstrated that one-third of patients with AKI in intensive care developed oliguria using a standardised definition of oliguria. Oliguric AKI was found to be significantly associated with higher rates of mortality from in-critical care through 1-year post-discharge.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 6\",\"pages\":\"sfaf170\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12203070/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf170\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf170","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Short- and long-term outcomes in oliguric and non-oliguric acute kidney injury in intensive care: a retrospective, post hoc, bicentric study.
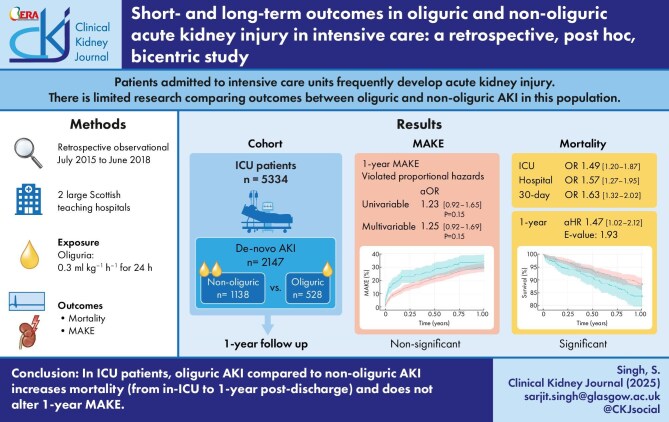
Background: Patients admitted to intensive care units (ICUs) frequently develop acute kidney injury (AKI). There is limited research comparing outcomes between oliguric and non-oliguric AKI in this population. This study aimed to investigate the short- and long-term outcomes in oliguric and non-oliguric AKI in intensive care patients; the specific outcomes assessed were mortality and major adverse kidney events. We hypothesised that short- and long-term outcomes would be poorer in oliguric compared with non-oliguric AKI in intensive care patients.
Methods: This retrospective observational cohort study utilised prospectively collected data routinely gathered during patients' admission. All adult patients >16 years of age admitted to two large Scottish general adult ICUs were included. Patients with long-term kidney replacement therapy, prior transplantation and ICU readmission were excluded. Oliguria was defined as urine output <0.3 ml/kg/h for 24 h. Outcomes were assessed using Cox proportional hazards analyses; should its assumptions be violated, odds ratios at prespecified time points were undertaken.
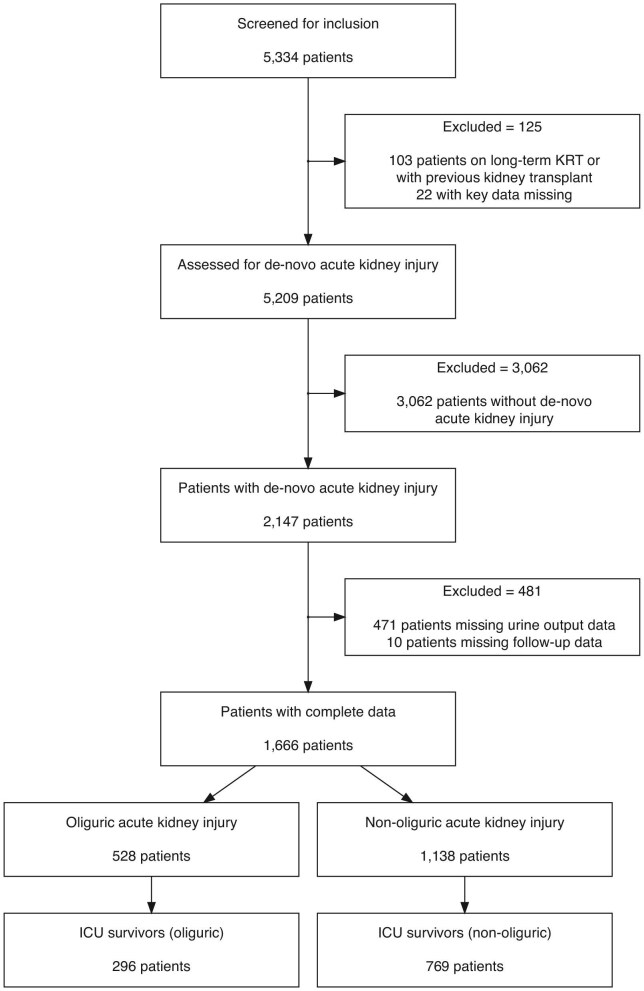
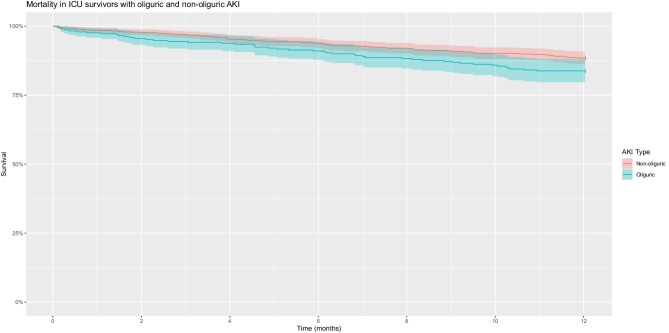
Results: Of the 2147 patients identified with de novo AKI, 1666 had sufficient urine output data for analysis. A total of 528 (31.7%) subjects had oliguric AKI lasting at least 24 h. The 1-year mortality was higher in oliguric patients [adjusted hazard ratio 1.45 (95% confidence interval 1.02-2.12), E-value 1.93]. Our data violated the proportional hazards assumption for major adverse kidney events; the 1-year odds ratio for major adverse renal events was non-significant at 1.25 (95% confidence interval 0.92-1.69).
Conclusion: Our study demonstrated that one-third of patients with AKI in intensive care developed oliguria using a standardised definition of oliguria. Oliguric AKI was found to be significantly associated with higher rates of mortality from in-critical care through 1-year post-discharge.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


