{"title":"一项多中心回顾性研究预测急性缺氧呼吸衰竭患者早期无创通气失败","authors":"Xiaoyi Liu, Hui Liu, Lijuan Chen, Xiangde Zheng, Hui Ran, Lili Chen, Rui Zhou, Yufeng Wang","doi":"10.1111/crj.70098","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Volume OXygenation (VOX) index has good efficacy in predicting the failure of high-flow nasal cannula therapy. However, its predictive value for treatment failure in patients receiving noninvasive ventilation (NIV) remains uncertain.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients who underwent early NIV treatment were grouped based on their 2-h NIV VOX Youden index. The low-risk group consisted of patients with a VOX value > 20.45 (<i>n</i> = 188), while the high-risk group included those with a VOX value ≤ 20.45 (<i>n</i> = 200). Baseline data and arterial blood gas values were collected at 2, 12, and 24 h after NIV initiation.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Compared to the low-risk group, the high-risk group exhibited higher SOFA scores, respiratory rates, and heart rates, along with a lower oxygenation index (P/F) (all <i>p</i> < 0.05). Following NIV treatment, the low-risk group showed a more significant increase in P/F values at 2 h, 12 h, and 24 h after NIV initiation. The low-risk group showed a lower VT and MV (minute ventilation volume) at 2 h, 12 h, and 24 h of NIV (<i>p</i> < 0.05). Moreover, the low-risk group had a lower intubation rate (7.98% vs. 77%, <i>p</i> < 0.05) and mortality rate (4.79% vs. 17.5%, <i>p</i> < 0.05). At 2 h of NIV, the area under the receiver operating characteristic curve for predicting NIV failure using the VOX index was 0.843 (95% CI 0.805–0.882). Using a VOX value threshold of 20.45 to predict NIV failure, the sensitivity was 69.1%, and the specificity was 94.4%. Furthermore, a VOX value ≤ 20.45 was identified as an independent risk factor for tracheal intubation and death.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>VOX index shows promise to serve as an effective evaluation index to predict early NIV efficacy in patients with AHRF; a VOX value > 20.45 after 2 h of NIV treatment can better predict improvements in hypoxia, respiratory drive, and NIV outcomes, guide early tracheal intubation in cases of NIV failure, and have a certain predictive effect on patient outcomes.</p>\n </section>\n </div>","PeriodicalId":55247,"journal":{"name":"Clinical Respiratory Journal","volume":"19 7","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/crj.70098","citationCount":"0","resultStr":"{\"title\":\"A Multicenter Retrospective Study Predicting Early Noninvasive Ventilation Failure in Patients With Acute Hypoxic Respiratory Failure\",\"authors\":\"Xiaoyi Liu, Hui Liu, Lijuan Chen, Xiangde Zheng, Hui Ran, Lili Chen, Rui Zhou, Yufeng Wang\",\"doi\":\"10.1111/crj.70098\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Volume OXygenation (VOX) index has good efficacy in predicting the failure of high-flow nasal cannula therapy. However, its predictive value for treatment failure in patients receiving noninvasive ventilation (NIV) remains uncertain.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Patients who underwent early NIV treatment were grouped based on their 2-h NIV VOX Youden index. The low-risk group consisted of patients with a VOX value > 20.45 (<i>n</i> = 188), while the high-risk group included those with a VOX value ≤ 20.45 (<i>n</i> = 200). Baseline data and arterial blood gas values were collected at 2, 12, and 24 h after NIV initiation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Compared to the low-risk group, the high-risk group exhibited higher SOFA scores, respiratory rates, and heart rates, along with a lower oxygenation index (P/F) (all <i>p</i> < 0.05). Following NIV treatment, the low-risk group showed a more significant increase in P/F values at 2 h, 12 h, and 24 h after NIV initiation. The low-risk group showed a lower VT and MV (minute ventilation volume) at 2 h, 12 h, and 24 h of NIV (<i>p</i> < 0.05). Moreover, the low-risk group had a lower intubation rate (7.98% vs. 77%, <i>p</i> < 0.05) and mortality rate (4.79% vs. 17.5%, <i>p</i> < 0.05). At 2 h of NIV, the area under the receiver operating characteristic curve for predicting NIV failure using the VOX index was 0.843 (95% CI 0.805–0.882). Using a VOX value threshold of 20.45 to predict NIV failure, the sensitivity was 69.1%, and the specificity was 94.4%. Furthermore, a VOX value ≤ 20.45 was identified as an independent risk factor for tracheal intubation and death.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>VOX index shows promise to serve as an effective evaluation index to predict early NIV efficacy in patients with AHRF; a VOX value > 20.45 after 2 h of NIV treatment can better predict improvements in hypoxia, respiratory drive, and NIV outcomes, guide early tracheal intubation in cases of NIV failure, and have a certain predictive effect on patient outcomes.</p>\\n </section>\\n </div>\",\"PeriodicalId\":55247,\"journal\":{\"name\":\"Clinical Respiratory Journal\",\"volume\":\"19 7\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-06-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/crj.70098\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Respiratory Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/crj.70098\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Respiratory Journal","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/crj.70098","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
A Multicenter Retrospective Study Predicting Early Noninvasive Ventilation Failure in Patients With Acute Hypoxic Respiratory Failure
Background
Volume OXygenation (VOX) index has good efficacy in predicting the failure of high-flow nasal cannula therapy. However, its predictive value for treatment failure in patients receiving noninvasive ventilation (NIV) remains uncertain.
Methods
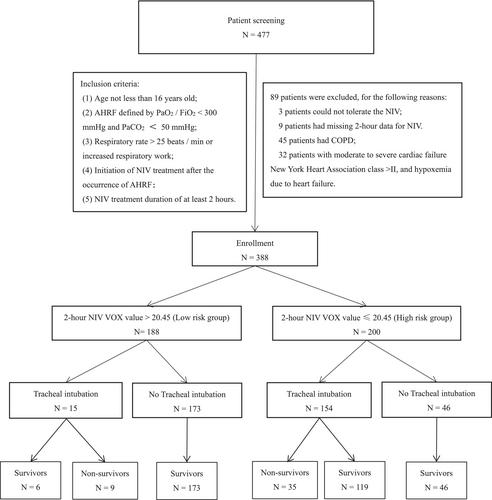
Patients who underwent early NIV treatment were grouped based on their 2-h NIV VOX Youden index. The low-risk group consisted of patients with a VOX value > 20.45 (n = 188), while the high-risk group included those with a VOX value ≤ 20.45 (n = 200). Baseline data and arterial blood gas values were collected at 2, 12, and 24 h after NIV initiation.
Results
Compared to the low-risk group, the high-risk group exhibited higher SOFA scores, respiratory rates, and heart rates, along with a lower oxygenation index (P/F) (all p < 0.05). Following NIV treatment, the low-risk group showed a more significant increase in P/F values at 2 h, 12 h, and 24 h after NIV initiation. The low-risk group showed a lower VT and MV (minute ventilation volume) at 2 h, 12 h, and 24 h of NIV (p < 0.05). Moreover, the low-risk group had a lower intubation rate (7.98% vs. 77%, p < 0.05) and mortality rate (4.79% vs. 17.5%, p < 0.05). At 2 h of NIV, the area under the receiver operating characteristic curve for predicting NIV failure using the VOX index was 0.843 (95% CI 0.805–0.882). Using a VOX value threshold of 20.45 to predict NIV failure, the sensitivity was 69.1%, and the specificity was 94.4%. Furthermore, a VOX value ≤ 20.45 was identified as an independent risk factor for tracheal intubation and death.
Conclusions
VOX index shows promise to serve as an effective evaluation index to predict early NIV efficacy in patients with AHRF; a VOX value > 20.45 after 2 h of NIV treatment can better predict improvements in hypoxia, respiratory drive, and NIV outcomes, guide early tracheal intubation in cases of NIV failure, and have a certain predictive effect on patient outcomes.
期刊介绍:
Overview
Effective with the 2016 volume, this journal will be published in an online-only format.
Aims and Scope
The Clinical Respiratory Journal (CRJ) provides a forum for clinical research in all areas of respiratory medicine from clinical lung disease to basic research relevant to the clinic.
We publish original research, review articles, case studies, editorials and book reviews in all areas of clinical lung disease including:
Asthma
Allergy
COPD
Non-invasive ventilation
Sleep related breathing disorders
Interstitial lung diseases
Lung cancer
Clinical genetics
Rhinitis
Airway and lung infection
Epidemiology
Pediatrics
CRJ provides a fast-track service for selected Phase II and Phase III trial studies.
Keywords
Clinical Respiratory Journal, respiratory, pulmonary, medicine, clinical, lung disease,
Abstracting and Indexing Information
Academic Search (EBSCO Publishing)
Academic Search Alumni Edition (EBSCO Publishing)
Embase (Elsevier)
Health & Medical Collection (ProQuest)
Health Research Premium Collection (ProQuest)
HEED: Health Economic Evaluations Database (Wiley-Blackwell)
Hospital Premium Collection (ProQuest)
Journal Citation Reports/Science Edition (Clarivate Analytics)
MEDLINE/PubMed (NLM)
ProQuest Central (ProQuest)
Science Citation Index Expanded (Clarivate Analytics)
SCOPUS (Elsevier)

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


