Constantin Unger, Felix Werner, Bettina Engel, Thomas Kühlein, Christoph Schulz, Christian Kümpel, Johannes Gorkotte, Susann Hueber
{"title":"重症监护后一年生存率作为全科医学预先护理指示的决策基础:149,144例患者的真实数据分析。","authors":"Constantin Unger, Felix Werner, Bettina Engel, Thomas Kühlein, Christoph Schulz, Christian Kümpel, Johannes Gorkotte, Susann Hueber","doi":"10.1371/journal.pone.0326031","DOIUrl":null,"url":null,"abstract":"<p><p>Providing counsel on advance care directives is challenging for general practitioners. Counselling is done on unknown future circumstances of possible critical illness and critical care in intensive care units. Following the principles of evidence-based medicine, the physician's task is to communicate evidence and elucidate the patient's position on it. However, suitable evidence of chances of survival in case of critical illness is lacking. Aim of this study was to generate long-term survival rates of patients receiving critical care as evidence for general practitioners who provide counselling for patients on advance care directives. We conducted a retrospective cohort study analysing one-year survival rates of critical care using German health insurance claims data from an anonymised nationwide health claims data pool of over five million German patients. All patients over 18 years of age receiving critical care for the first time were included.Main outcome of our study were one-year survival probabilities depending on age and on acute life prolonging procedures. Procedures analysed were non-invasive and invasive mechanical ventilation (nMV, iMV), renal replacement therapy (RRT), their combinations (nMV + RRT, iMV + RRT), and cardiopulmonary resuscitation (CPR). A total of 149,144 datasets was analysed. One-year survival probability of all patients was 77.5%. Survival rates ranged from 94.5% in patients under 50 without any further acute life prolonging procedures to 16.4% in those older than 80 who received iMV + RRT. The application of at least one procedure was associated with an increased risk of death (HR 3.06, 95% CI 2.99 to 3.12) as was CPR (HR 4.22, 95% CI 4.07 to 4.37). Differences between pre- and COVID periods were modest. To enable patient's decision-making in creating advance care directives, our results provide easily applicable external evidence for general practitioners counselling on advance care directives by providing probabilities of survival in critical care.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 6","pages":"e0326031"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204473/pdf/","citationCount":"0","resultStr":"{\"title\":\"One-year survival after critical care as a decision basis for advance care directives in general medicine: Real word data analysis of 149,144 patients.\",\"authors\":\"Constantin Unger, Felix Werner, Bettina Engel, Thomas Kühlein, Christoph Schulz, Christian Kümpel, Johannes Gorkotte, Susann Hueber\",\"doi\":\"10.1371/journal.pone.0326031\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Providing counsel on advance care directives is challenging for general practitioners. Counselling is done on unknown future circumstances of possible critical illness and critical care in intensive care units. Following the principles of evidence-based medicine, the physician's task is to communicate evidence and elucidate the patient's position on it. However, suitable evidence of chances of survival in case of critical illness is lacking. Aim of this study was to generate long-term survival rates of patients receiving critical care as evidence for general practitioners who provide counselling for patients on advance care directives. We conducted a retrospective cohort study analysing one-year survival rates of critical care using German health insurance claims data from an anonymised nationwide health claims data pool of over five million German patients. All patients over 18 years of age receiving critical care for the first time were included.Main outcome of our study were one-year survival probabilities depending on age and on acute life prolonging procedures. Procedures analysed were non-invasive and invasive mechanical ventilation (nMV, iMV), renal replacement therapy (RRT), their combinations (nMV + RRT, iMV + RRT), and cardiopulmonary resuscitation (CPR). A total of 149,144 datasets was analysed. One-year survival probability of all patients was 77.5%. Survival rates ranged from 94.5% in patients under 50 without any further acute life prolonging procedures to 16.4% in those older than 80 who received iMV + RRT. The application of at least one procedure was associated with an increased risk of death (HR 3.06, 95% CI 2.99 to 3.12) as was CPR (HR 4.22, 95% CI 4.07 to 4.37). Differences between pre- and COVID periods were modest. To enable patient's decision-making in creating advance care directives, our results provide easily applicable external evidence for general practitioners counselling on advance care directives by providing probabilities of survival in critical care.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 6\",\"pages\":\"e0326031\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-06-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12204473/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0326031\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0326031","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
摘要
对全科医生来说,为预先护理指示提供咨询是一项挑战。就未来可能出现的危重疾病和重症监护的未知情况提供咨询。遵循循证医学的原则,医生的任务是传达证据并阐明患者的立场。然而,缺乏在危急情况下生存机会的适当证据。本研究的目的是产生长期生存率的病人接受重症监护作为证据,为全科医生提供咨询的病人预先护理指示。我们进行了一项回顾性队列研究,使用来自500多万德国患者的匿名全国健康索赔数据库的德国健康保险索赔数据,分析重症监护患者的一年生存率。所有18岁以上首次接受重症监护的患者均被纳入。我们研究的主要结果是一年生存率取决于年龄和急性生命延长手术。分析的程序包括无创和有创机械通气(nMV、iMV)、肾脏替代疗法(RRT)及其联合(nMV + RRT、iMV + RRT)和心肺复苏(CPR)。共分析了149,144个数据集。所有患者1年生存率为77.5%。50岁以下未接受任何急性延长生命手术的患者生存率为94.5%,80岁以上接受iMV + RRT的患者生存率为16.4%。应用至少一种手术与死亡风险增加相关(HR 3.06, 95% CI 2.99 ~ 3.12),心肺复苏术(HR 4.22, 95% CI 4.07 ~ 4.37)也是如此。COVID前和COVID期间的差异不大。为了使患者在制定预先护理指令时能够做出决策,我们的研究结果通过提供危重护理的生存概率,为全科医生提供预先护理指令咨询提供了容易适用的外部证据。
One-year survival after critical care as a decision basis for advance care directives in general medicine: Real word data analysis of 149,144 patients.
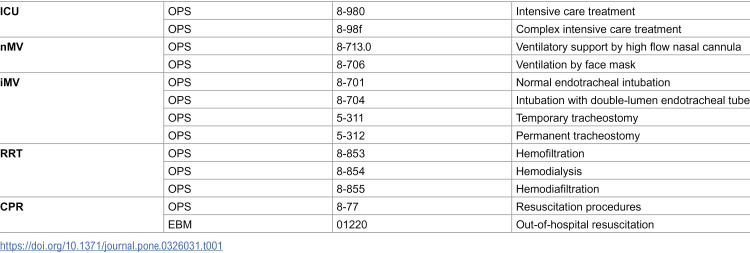
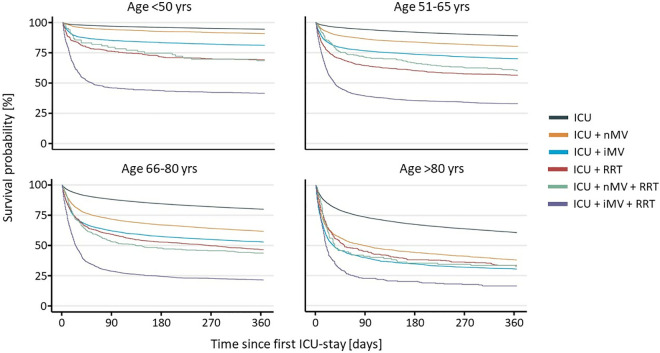
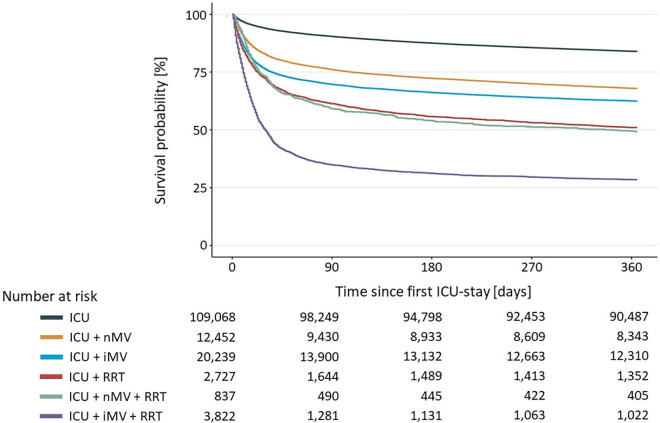
Providing counsel on advance care directives is challenging for general practitioners. Counselling is done on unknown future circumstances of possible critical illness and critical care in intensive care units. Following the principles of evidence-based medicine, the physician's task is to communicate evidence and elucidate the patient's position on it. However, suitable evidence of chances of survival in case of critical illness is lacking. Aim of this study was to generate long-term survival rates of patients receiving critical care as evidence for general practitioners who provide counselling for patients on advance care directives. We conducted a retrospective cohort study analysing one-year survival rates of critical care using German health insurance claims data from an anonymised nationwide health claims data pool of over five million German patients. All patients over 18 years of age receiving critical care for the first time were included.Main outcome of our study were one-year survival probabilities depending on age and on acute life prolonging procedures. Procedures analysed were non-invasive and invasive mechanical ventilation (nMV, iMV), renal replacement therapy (RRT), their combinations (nMV + RRT, iMV + RRT), and cardiopulmonary resuscitation (CPR). A total of 149,144 datasets was analysed. One-year survival probability of all patients was 77.5%. Survival rates ranged from 94.5% in patients under 50 without any further acute life prolonging procedures to 16.4% in those older than 80 who received iMV + RRT. The application of at least one procedure was associated with an increased risk of death (HR 3.06, 95% CI 2.99 to 3.12) as was CPR (HR 4.22, 95% CI 4.07 to 4.37). Differences between pre- and COVID periods were modest. To enable patient's decision-making in creating advance care directives, our results provide easily applicable external evidence for general practitioners counselling on advance care directives by providing probabilities of survival in critical care.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


