Kathleen Perry, Miko Yu, Joel T Adler, Lindsey M Maclay, David C Cron, Sumit Mohan, Syed A Husain
{"title":"私人保险和活体肾移植之间的关系:平价医疗法案作为一个自然实验。","authors":"Kathleen Perry, Miko Yu, Joel T Adler, Lindsey M Maclay, David C Cron, Sumit Mohan, Syed A Husain","doi":"10.5527/wjn.v14.i2.101419","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Private insurance coverage is associated with higher rates of living donor kidney transplantation (LDKT) but whether this is attributable to confounding is not known.</p><p><strong>Aim: </strong>To study the association between increased access to private health insurance and LDKT.</p><p><strong>Methods: </strong>Retrospective cohort study using United States transplant registry data. We identified incident candidates aged 22-29 years who were waitlisted for a kidney-only transplant from 2005-2014, excluding prior transplant recipients and those with missing data. We calculated the hazard of LDKT after waitlisting for those with private insurance <i>vs</i> other insurance pre-Affordable Care Act (ACA) <i>vs</i> post-ACA, using death and delisting as competing events, for candidates affected by the policy change (age 22-25 years) <i>vs</i> those who were not (age 26-29 years).</p><p><strong>Results: </strong>A total of 13817 candidates were included, of whom 46% were age 22-25 years and 54% were age 26-29 years. Among candidates aged 22-25 years at listing, those listed post-ACA were more likely to have private insurance compared to those listed pre-ACA (42% <i>vs</i> 35%), but there was no difference in private insurance coverage between eras among candidates aged 26-29 years at listing. In adjusted competing risk regression, privately insured patients age 22-25 years were less likely to receive a LDKT post-ACA compared to pre-ACA [hazard ratio (HR) = 0.88, 95%CI: 0.78-1.00], as were those aged 22-25 years old with other insurance types (HR = 0.80, 95%CI: 0.69-0.92). These associations were not seen among candidates age 26-29 years.</p><p><strong>Conclusion: </strong>Candidates age 22-25 years were likelier to have private insurance post-ACA, without an increased rate in LDKT. Demonstrations of associations between insurance and LDKT are likely attributable to residual confounding.</p>","PeriodicalId":94272,"journal":{"name":"World journal of nephrology","volume":"14 2","pages":"101419"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001229/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between private insurance and living donor kidney transplant: Affordable Care Act as a natural experiment.\",\"authors\":\"Kathleen Perry, Miko Yu, Joel T Adler, Lindsey M Maclay, David C Cron, Sumit Mohan, Syed A Husain\",\"doi\":\"10.5527/wjn.v14.i2.101419\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Private insurance coverage is associated with higher rates of living donor kidney transplantation (LDKT) but whether this is attributable to confounding is not known.</p><p><strong>Aim: </strong>To study the association between increased access to private health insurance and LDKT.</p><p><strong>Methods: </strong>Retrospective cohort study using United States transplant registry data. We identified incident candidates aged 22-29 years who were waitlisted for a kidney-only transplant from 2005-2014, excluding prior transplant recipients and those with missing data. We calculated the hazard of LDKT after waitlisting for those with private insurance <i>vs</i> other insurance pre-Affordable Care Act (ACA) <i>vs</i> post-ACA, using death and delisting as competing events, for candidates affected by the policy change (age 22-25 years) <i>vs</i> those who were not (age 26-29 years).</p><p><strong>Results: </strong>A total of 13817 candidates were included, of whom 46% were age 22-25 years and 54% were age 26-29 years. Among candidates aged 22-25 years at listing, those listed post-ACA were more likely to have private insurance compared to those listed pre-ACA (42% <i>vs</i> 35%), but there was no difference in private insurance coverage between eras among candidates aged 26-29 years at listing. In adjusted competing risk regression, privately insured patients age 22-25 years were less likely to receive a LDKT post-ACA compared to pre-ACA [hazard ratio (HR) = 0.88, 95%CI: 0.78-1.00], as were those aged 22-25 years old with other insurance types (HR = 0.80, 95%CI: 0.69-0.92). These associations were not seen among candidates age 26-29 years.</p><p><strong>Conclusion: </strong>Candidates age 22-25 years were likelier to have private insurance post-ACA, without an increased rate in LDKT. Demonstrations of associations between insurance and LDKT are likely attributable to residual confounding.</p>\",\"PeriodicalId\":94272,\"journal\":{\"name\":\"World journal of nephrology\",\"volume\":\"14 2\",\"pages\":\"101419\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12001229/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5527/wjn.v14.i2.101419\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v14.i2.101419","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Association between private insurance and living donor kidney transplant: Affordable Care Act as a natural experiment.
Background: Private insurance coverage is associated with higher rates of living donor kidney transplantation (LDKT) but whether this is attributable to confounding is not known.
Aim: To study the association between increased access to private health insurance and LDKT.
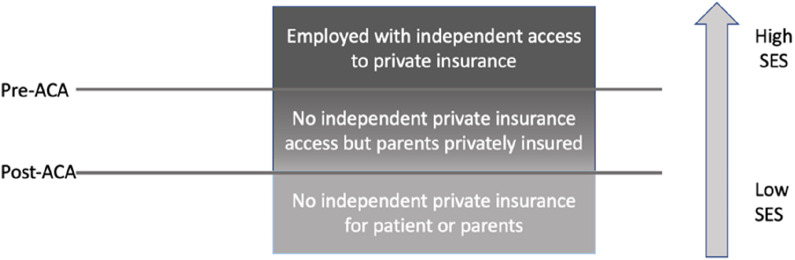
Methods: Retrospective cohort study using United States transplant registry data. We identified incident candidates aged 22-29 years who were waitlisted for a kidney-only transplant from 2005-2014, excluding prior transplant recipients and those with missing data. We calculated the hazard of LDKT after waitlisting for those with private insurance vs other insurance pre-Affordable Care Act (ACA) vs post-ACA, using death and delisting as competing events, for candidates affected by the policy change (age 22-25 years) vs those who were not (age 26-29 years).
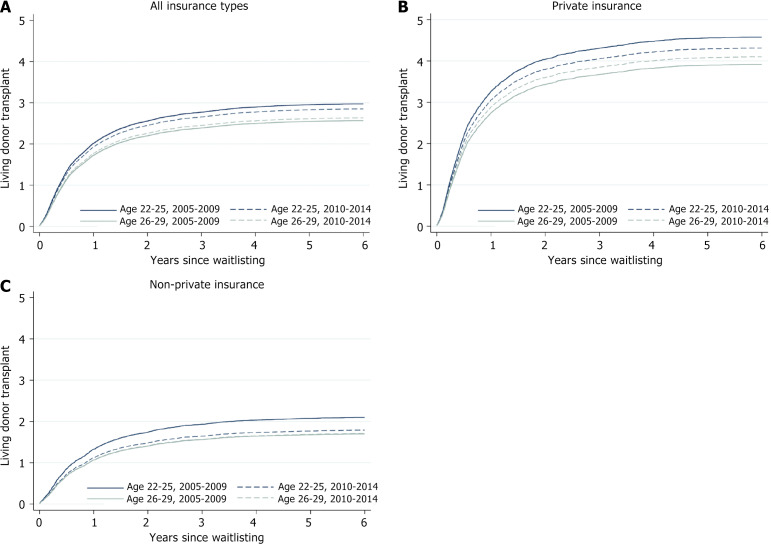
Results: A total of 13817 candidates were included, of whom 46% were age 22-25 years and 54% were age 26-29 years. Among candidates aged 22-25 years at listing, those listed post-ACA were more likely to have private insurance compared to those listed pre-ACA (42% vs 35%), but there was no difference in private insurance coverage between eras among candidates aged 26-29 years at listing. In adjusted competing risk regression, privately insured patients age 22-25 years were less likely to receive a LDKT post-ACA compared to pre-ACA [hazard ratio (HR) = 0.88, 95%CI: 0.78-1.00], as were those aged 22-25 years old with other insurance types (HR = 0.80, 95%CI: 0.69-0.92). These associations were not seen among candidates age 26-29 years.
Conclusion: Candidates age 22-25 years were likelier to have private insurance post-ACA, without an increased rate in LDKT. Demonstrations of associations between insurance and LDKT are likely attributable to residual confounding.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


