Mintesnot T Teni, Travis Loux, Ness Sandoval, Anne Sebert Kuhlmann
{"title":"检查埃塞俄比亚LARC的低吸收:对个人水平易感因素和促成因素的分析。","authors":"Mintesnot T Teni, Travis Loux, Ness Sandoval, Anne Sebert Kuhlmann","doi":"10.3389/fgwh.2025.1547891","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>According to the 2019 Ethiopian Demographic and Health Survey (EDHS) only 11% of married reproductive-age women in Ethiopia use long-acting reversible contraceptives (LARCs). This study aimed to identify individual characteristics associated with LARC uptake compared to short-acting contraceptives, traditional and barrier methods, and non-contraceptive use.</p><p><strong>Methods: </strong>Data from the 2019 Performance Monitoring for Action (PMA) Ethiopia survey (<i>n</i> = 8,182) were used to run multilevel logistic regression models. The sample includes sexually active reproductive-age women (15-49 years). Independent variables were grouped into predisposing and enabling factors guided by the Andersen Behavioral Model of Health Services.</p><p><strong>Results: </strong>LARC uptake in this study was 9.7%. Older, single, nulliparous, and Muslim women had lower LARC use than non-contraceptive and traditional/barrier method use. When compared to short-acting method use, low LARC use was associated with smaller household size and no exposure to family planning information. When compared to all other groups, contraceptive autonomy was associated with higher LARC uptake. Younger women and women living in rural areas were less likely to use IUDs than implants.</p><p><strong>Discussion: </strong>Policymakers could use these findings to tailor interventions to specific populations with low LARC uptake. Training providers on counseling and LARC eligibility could help improve LARC uptake among populations, including less-empowered women. Involving religious leaders in contraceptive health education has the potential to increase LARC use.</p>","PeriodicalId":73087,"journal":{"name":"Frontiers in global women's health","volume":"6 ","pages":"1547891"},"PeriodicalIF":2.4000,"publicationDate":"2025-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179146/pdf/","citationCount":"0","resultStr":"{\"title\":\"Examining the low uptake of LARC in Ethiopia: an analysis of individual-level predisposing and enabling factors.\",\"authors\":\"Mintesnot T Teni, Travis Loux, Ness Sandoval, Anne Sebert Kuhlmann\",\"doi\":\"10.3389/fgwh.2025.1547891\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>According to the 2019 Ethiopian Demographic and Health Survey (EDHS) only 11% of married reproductive-age women in Ethiopia use long-acting reversible contraceptives (LARCs). This study aimed to identify individual characteristics associated with LARC uptake compared to short-acting contraceptives, traditional and barrier methods, and non-contraceptive use.</p><p><strong>Methods: </strong>Data from the 2019 Performance Monitoring for Action (PMA) Ethiopia survey (<i>n</i> = 8,182) were used to run multilevel logistic regression models. The sample includes sexually active reproductive-age women (15-49 years). Independent variables were grouped into predisposing and enabling factors guided by the Andersen Behavioral Model of Health Services.</p><p><strong>Results: </strong>LARC uptake in this study was 9.7%. Older, single, nulliparous, and Muslim women had lower LARC use than non-contraceptive and traditional/barrier method use. When compared to short-acting method use, low LARC use was associated with smaller household size and no exposure to family planning information. When compared to all other groups, contraceptive autonomy was associated with higher LARC uptake. Younger women and women living in rural areas were less likely to use IUDs than implants.</p><p><strong>Discussion: </strong>Policymakers could use these findings to tailor interventions to specific populations with low LARC uptake. Training providers on counseling and LARC eligibility could help improve LARC uptake among populations, including less-empowered women. Involving religious leaders in contraceptive health education has the potential to increase LARC use.</p>\",\"PeriodicalId\":73087,\"journal\":{\"name\":\"Frontiers in global women's health\",\"volume\":\"6 \",\"pages\":\"1547891\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-06-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179146/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in global women's health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/fgwh.2025.1547891\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in global women's health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fgwh.2025.1547891","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Examining the low uptake of LARC in Ethiopia: an analysis of individual-level predisposing and enabling factors.
Introduction: According to the 2019 Ethiopian Demographic and Health Survey (EDHS) only 11% of married reproductive-age women in Ethiopia use long-acting reversible contraceptives (LARCs). This study aimed to identify individual characteristics associated with LARC uptake compared to short-acting contraceptives, traditional and barrier methods, and non-contraceptive use.
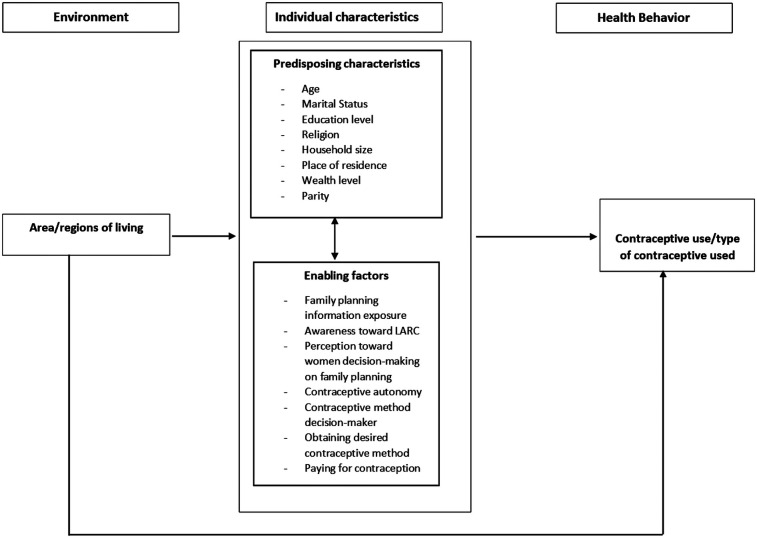
Methods: Data from the 2019 Performance Monitoring for Action (PMA) Ethiopia survey (n = 8,182) were used to run multilevel logistic regression models. The sample includes sexually active reproductive-age women (15-49 years). Independent variables were grouped into predisposing and enabling factors guided by the Andersen Behavioral Model of Health Services.
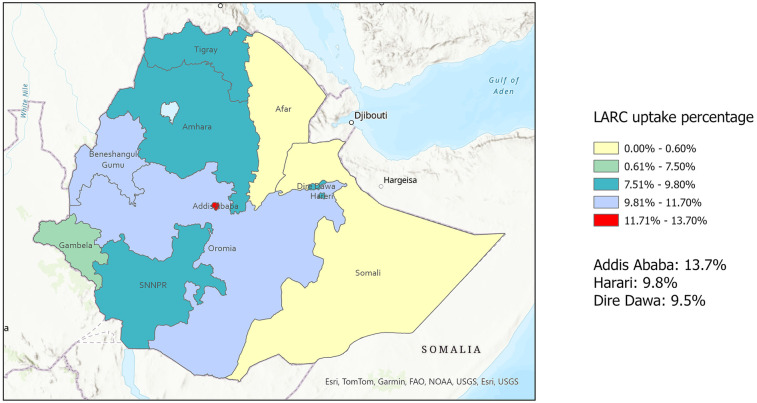
Results: LARC uptake in this study was 9.7%. Older, single, nulliparous, and Muslim women had lower LARC use than non-contraceptive and traditional/barrier method use. When compared to short-acting method use, low LARC use was associated with smaller household size and no exposure to family planning information. When compared to all other groups, contraceptive autonomy was associated with higher LARC uptake. Younger women and women living in rural areas were less likely to use IUDs than implants.
Discussion: Policymakers could use these findings to tailor interventions to specific populations with low LARC uptake. Training providers on counseling and LARC eligibility could help improve LARC uptake among populations, including less-empowered women. Involving religious leaders in contraceptive health education has the potential to increase LARC use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


