{"title":"推进止血:一项针对非静脉曲张上消化道出血的新型与传统内镜治疗的荟萃分析。","authors":"Shivangini Duggal, Ishana Kalra, Keisha Kalra, Vicky Bhagat","doi":"10.4253/wjge.v17.i6.107142","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non variceal upper gastrointestinal bleeding (NVUGIB) is a life-threatening condition requiring prompt and effective hemostasis. Various endoscopic interventions, including novel hemostatic powders (HP), over-the-scope clips (OTSC), and traditional approaches, have been employed to manage upper gastrointestinal bleeding (UGIB). Despite advancements, comparative efficacy and safety of these modalities remain uncertain.</p><p><strong>Aim: </strong>To evaluate the efficacy and safety of novel hemostatic interventions compared to conventional endoscopic techniques for managing UGIB.</p><p><strong>Methods: </strong>Cochrane, MEDLINE, PubMed and Scopus libraries were searched for randomized controlled trials (RCTs) published up to October 2024. Only RCTs comparing novel interventions, such as HP or OTSC, with conventional endoscopic treatments computed tomography (CT) were included. The primary outcome was the 30-day rebleeding rate. Secondary outcomes included initial hemostasis, short-term rebleeding rates, need for salvage therapy (surgical/angiographic), 30-day all-cause mortality, and bleeding-related mortality. We performed pairwise and network meta- analyses for all treatments.</p><p><strong>Results: </strong>Seventeen studies were included in this analysis. Regarding the 30-day rebleeding rate, OTSC and HP showed superior efficacy compared with CT [OTSC <i>vs</i> CT: Relative risk (RR): 0.47, 95% confidence interval (CI): 0.33-0.65; HP <i>vs</i> CT: RR: 0.73, 95%CI: 0.45-1.13], while OTSC and HP had comparable efficacy (RR: 0.56, 95%CI: 0.30-1.05). OTSC ranked the highest in the network ranking estimate for this outcome. For the secondary outcomes, OTSC demonstrated superior efficacy for the short-term rebleeding rate (OTSC <i>vs</i> CT: RR: 0.35, 95%CI: 0.14-0.74; HP <i>vs</i> CT: RR: 0.62, 95%CI: 0.28-1.35; OTSC <i>vs</i> HP: RR: 0.59, 95%CI: 0.17-1.67). Regarding the initial hemostasis rate, OTSC was slightly more effective than CT (OTSC <i>vs</i> CT: RR: 1.20, 95%CI: 1.06-1.57) and comparable to HP (OTSC <i>vs</i> HP: RR: 1.08, 95%CI: 0.89-1.40). There were no significant differences among treatments for all-cause mortality, bleeding-related mortality, or the necessity of surgical or angiographic salvage therapy. OTSC consistently ranked highest across most outcomes in the network ranking estimate.</p><p><strong>Conclusion: </strong>This meta-analysis highlights OTSC as the most effective intervention for reducing 30-day and short-term rebleeding rates in NVUGIB, surpassing both CT and HP, supporting OTSC as a preferred first-line treatment for NVUGIB, while HP and CT remain viable alternatives. Further studies are needed to explore long-term outcomes and cost-effectiveness.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"17 6","pages":"107142"},"PeriodicalIF":1.8000,"publicationDate":"2025-06-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179957/pdf/","citationCount":"0","resultStr":"{\"title\":\"Advancing hemostasis: A meta-analysis of novel <i>vs</i> conventional endoscopic therapies for non variceal upper gastrointestinal bleeding.\",\"authors\":\"Shivangini Duggal, Ishana Kalra, Keisha Kalra, Vicky Bhagat\",\"doi\":\"10.4253/wjge.v17.i6.107142\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Non variceal upper gastrointestinal bleeding (NVUGIB) is a life-threatening condition requiring prompt and effective hemostasis. Various endoscopic interventions, including novel hemostatic powders (HP), over-the-scope clips (OTSC), and traditional approaches, have been employed to manage upper gastrointestinal bleeding (UGIB). Despite advancements, comparative efficacy and safety of these modalities remain uncertain.</p><p><strong>Aim: </strong>To evaluate the efficacy and safety of novel hemostatic interventions compared to conventional endoscopic techniques for managing UGIB.</p><p><strong>Methods: </strong>Cochrane, MEDLINE, PubMed and Scopus libraries were searched for randomized controlled trials (RCTs) published up to October 2024. Only RCTs comparing novel interventions, such as HP or OTSC, with conventional endoscopic treatments computed tomography (CT) were included. The primary outcome was the 30-day rebleeding rate. Secondary outcomes included initial hemostasis, short-term rebleeding rates, need for salvage therapy (surgical/angiographic), 30-day all-cause mortality, and bleeding-related mortality. We performed pairwise and network meta- analyses for all treatments.</p><p><strong>Results: </strong>Seventeen studies were included in this analysis. Regarding the 30-day rebleeding rate, OTSC and HP showed superior efficacy compared with CT [OTSC <i>vs</i> CT: Relative risk (RR): 0.47, 95% confidence interval (CI): 0.33-0.65; HP <i>vs</i> CT: RR: 0.73, 95%CI: 0.45-1.13], while OTSC and HP had comparable efficacy (RR: 0.56, 95%CI: 0.30-1.05). OTSC ranked the highest in the network ranking estimate for this outcome. For the secondary outcomes, OTSC demonstrated superior efficacy for the short-term rebleeding rate (OTSC <i>vs</i> CT: RR: 0.35, 95%CI: 0.14-0.74; HP <i>vs</i> CT: RR: 0.62, 95%CI: 0.28-1.35; OTSC <i>vs</i> HP: RR: 0.59, 95%CI: 0.17-1.67). Regarding the initial hemostasis rate, OTSC was slightly more effective than CT (OTSC <i>vs</i> CT: RR: 1.20, 95%CI: 1.06-1.57) and comparable to HP (OTSC <i>vs</i> HP: RR: 1.08, 95%CI: 0.89-1.40). There were no significant differences among treatments for all-cause mortality, bleeding-related mortality, or the necessity of surgical or angiographic salvage therapy. OTSC consistently ranked highest across most outcomes in the network ranking estimate.</p><p><strong>Conclusion: </strong>This meta-analysis highlights OTSC as the most effective intervention for reducing 30-day and short-term rebleeding rates in NVUGIB, surpassing both CT and HP, supporting OTSC as a preferred first-line treatment for NVUGIB, while HP and CT remain viable alternatives. Further studies are needed to explore long-term outcomes and cost-effectiveness.</p>\",\"PeriodicalId\":23953,\"journal\":{\"name\":\"World Journal of Gastrointestinal Endoscopy\",\"volume\":\"17 6\",\"pages\":\"107142\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-06-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179957/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4253/wjge.v17.i6.107142\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v17.i6.107142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:非静脉曲张性上消化道出血(NVUGIB)是一种危及生命的疾病,需要及时有效的止血。各种内镜干预措施,包括新型止血粉(HP)、镜外夹(OTSC)和传统方法,已被用于治疗上消化道出血(UGIB)。尽管取得了进展,但这些方法的相对疗效和安全性仍然不确定。目的:评价新型止血干预与传统内镜治疗UGIB的疗效和安全性。方法:检索Cochrane、MEDLINE、PubMed和Scopus数据库,检索截至2024年10月发表的随机对照试验(rct)。仅纳入比较新型干预措施(如HP或OTSC)与传统内窥镜治疗(计算机断层扫描(CT))的随机对照试验。主要观察指标为30天再出血率。次要结局包括初始止血、短期再出血率、需要补救性治疗(手术/血管造影)、30天全因死亡率和出血相关死亡率。我们对所有治疗进行了两两和网络meta分析。结果:本分析纳入了17项研究。关于30天再出血率,OTSC和HP的疗效优于CT [OTSC vs CT:相对风险(RR): 0.47, 95%可信区间(CI): 0.33-0.65;HP vs CT: RR: 0.73, 95%CI: 0.45-1.13],而OTSC和HP的疗效相当(RR: 0.56, 95%CI: 0.30-1.05)。OTSC在该结果的网络排名估计中排名最高。次要结局方面,OTSC在短期再出血率方面表现出优越的疗效(OTSC vs CT: RR: 0.35, 95%CI: 0.14-0.74;HP vs CT: RR: 0.62, 95%CI: 0.28-1.35;OTSC vs HP: RR: 0.59, 95%CI: 0.17-1.67)。在初始止血率方面,OTSC略高于CT (OTSC vs CT: RR: 1.20, 95%CI: 1.06-1.57),与HP相当(OTSC vs HP: RR: 1.08, 95%CI: 0.89-1.40)。在全因死亡率、出血相关死亡率、手术或血管造影治疗的必要性方面,治疗方法没有显著差异。在网络排名估计中,OTSC在大多数结果中始终排名最高。结论:该荟萃分析强调OTSC是降低NVUGIB患者30天和短期再出血率的最有效干预措施,超过了CT和HP,支持OTSC作为NVUGIB首选一线治疗,而HP和CT仍然是可行的替代方案。需要进一步的研究来探索长期结果和成本效益。
Advancing hemostasis: A meta-analysis of novel vs conventional endoscopic therapies for non variceal upper gastrointestinal bleeding.
Background: Non variceal upper gastrointestinal bleeding (NVUGIB) is a life-threatening condition requiring prompt and effective hemostasis. Various endoscopic interventions, including novel hemostatic powders (HP), over-the-scope clips (OTSC), and traditional approaches, have been employed to manage upper gastrointestinal bleeding (UGIB). Despite advancements, comparative efficacy and safety of these modalities remain uncertain.
Aim: To evaluate the efficacy and safety of novel hemostatic interventions compared to conventional endoscopic techniques for managing UGIB.
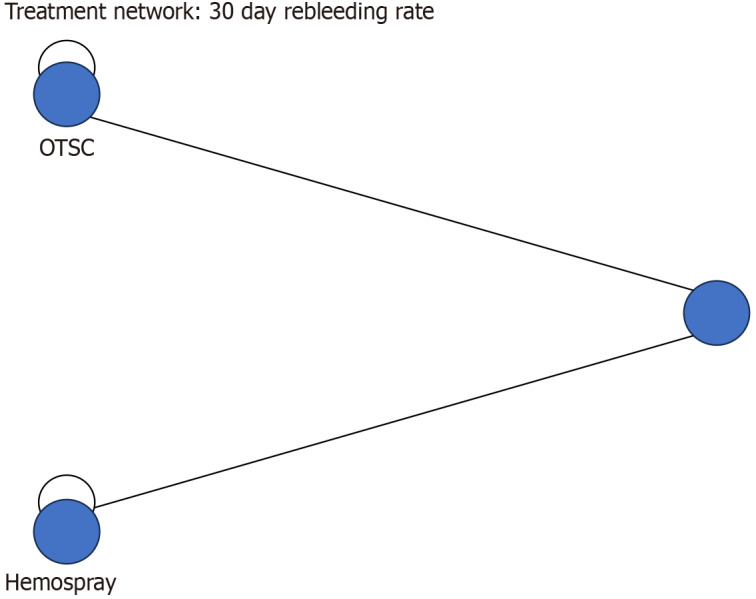
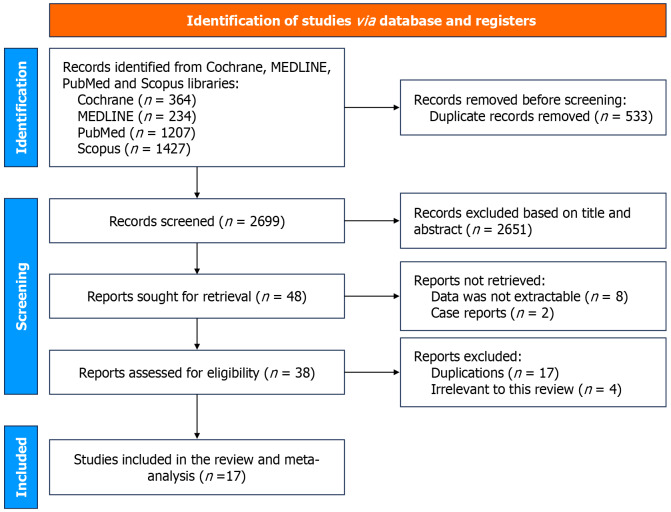
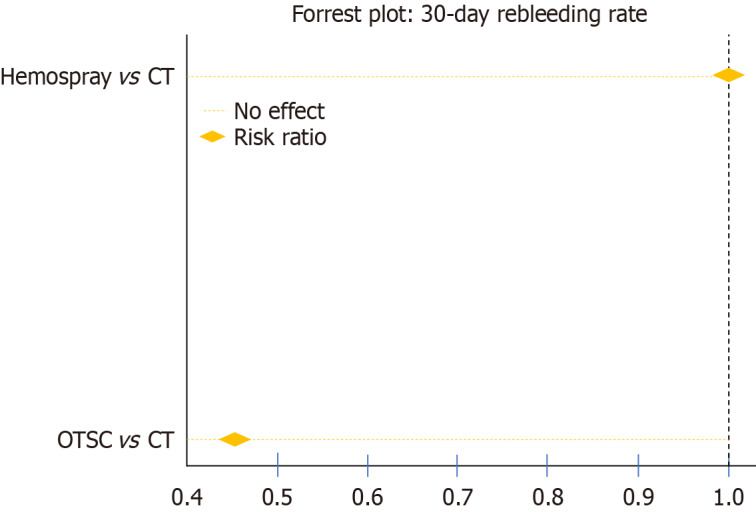
Methods: Cochrane, MEDLINE, PubMed and Scopus libraries were searched for randomized controlled trials (RCTs) published up to October 2024. Only RCTs comparing novel interventions, such as HP or OTSC, with conventional endoscopic treatments computed tomography (CT) were included. The primary outcome was the 30-day rebleeding rate. Secondary outcomes included initial hemostasis, short-term rebleeding rates, need for salvage therapy (surgical/angiographic), 30-day all-cause mortality, and bleeding-related mortality. We performed pairwise and network meta- analyses for all treatments.
Results: Seventeen studies were included in this analysis. Regarding the 30-day rebleeding rate, OTSC and HP showed superior efficacy compared with CT [OTSC vs CT: Relative risk (RR): 0.47, 95% confidence interval (CI): 0.33-0.65; HP vs CT: RR: 0.73, 95%CI: 0.45-1.13], while OTSC and HP had comparable efficacy (RR: 0.56, 95%CI: 0.30-1.05). OTSC ranked the highest in the network ranking estimate for this outcome. For the secondary outcomes, OTSC demonstrated superior efficacy for the short-term rebleeding rate (OTSC vs CT: RR: 0.35, 95%CI: 0.14-0.74; HP vs CT: RR: 0.62, 95%CI: 0.28-1.35; OTSC vs HP: RR: 0.59, 95%CI: 0.17-1.67). Regarding the initial hemostasis rate, OTSC was slightly more effective than CT (OTSC vs CT: RR: 1.20, 95%CI: 1.06-1.57) and comparable to HP (OTSC vs HP: RR: 1.08, 95%CI: 0.89-1.40). There were no significant differences among treatments for all-cause mortality, bleeding-related mortality, or the necessity of surgical or angiographic salvage therapy. OTSC consistently ranked highest across most outcomes in the network ranking estimate.
Conclusion: This meta-analysis highlights OTSC as the most effective intervention for reducing 30-day and short-term rebleeding rates in NVUGIB, surpassing both CT and HP, supporting OTSC as a preferred first-line treatment for NVUGIB, while HP and CT remain viable alternatives. Further studies are needed to explore long-term outcomes and cost-effectiveness.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


