Sho Akita, Akinori Tamenishi, Yasumoto Matsumura, Kunihiro Maruyama, Jun Ito
{"title":"a型主动脉夹层合并肠系膜灌注不良患者在中央主动脉修复前成功行紧急脏支支架置入1例。","authors":"Sho Akita, Akinori Tamenishi, Yasumoto Matsumura, Kunihiro Maruyama, Jun Ito","doi":"10.70352/scrj.cr.25-0136","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Stanford Type A acute aortic dissection (AAD) complicated by mesenteric malperfusion has a mortality rate exceeding 60%. Conventional immediate central aortic repair may be inadequate in such complex cases. Emerging evidence suggests that a staged approach may improve outcomes.</p><p><strong>Case presentation: </strong>A 71-year-old male presented with acute chest pain and was diagnosed with Stanford Type A AAD extending to the abdominal aorta, with superior mesenteric artery (SMA) dissection leading to intestinal ischemia. To restore intestinal perfusion, emergency endovascular SMA stenting was performed as the initial intervention, followed by ascending aorta and total arch replacement using the frozen elephant trunk technique 12 hours later. The patient recovered without complications and was discharged ambulatory on postoperative day 20.</p><p><strong>Conclusions: </strong>This case highlights the efficacy of a staged approach prioritizing mesenteric revascularization before central aortic repair in AAD complicated by visceral malperfusion. By first addressing end-organ ischemia, we potentially mitigated the risk of irreversible bowel necrosis while enabling subsequent central aortic repair. Our experience adds to the growing body of evidence supporting individualized, pathophysiology-guided treatment strategies for this challenging clinical scenario.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179782/pdf/","citationCount":"0","resultStr":"{\"title\":\"Successful Emergency Stenting of a Visceral Branch Prior to Central Aortic Repair in Type A Aortic Dissection with Mesenteric Malperfusion: A Case Report.\",\"authors\":\"Sho Akita, Akinori Tamenishi, Yasumoto Matsumura, Kunihiro Maruyama, Jun Ito\",\"doi\":\"10.70352/scrj.cr.25-0136\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Stanford Type A acute aortic dissection (AAD) complicated by mesenteric malperfusion has a mortality rate exceeding 60%. Conventional immediate central aortic repair may be inadequate in such complex cases. Emerging evidence suggests that a staged approach may improve outcomes.</p><p><strong>Case presentation: </strong>A 71-year-old male presented with acute chest pain and was diagnosed with Stanford Type A AAD extending to the abdominal aorta, with superior mesenteric artery (SMA) dissection leading to intestinal ischemia. To restore intestinal perfusion, emergency endovascular SMA stenting was performed as the initial intervention, followed by ascending aorta and total arch replacement using the frozen elephant trunk technique 12 hours later. The patient recovered without complications and was discharged ambulatory on postoperative day 20.</p><p><strong>Conclusions: </strong>This case highlights the efficacy of a staged approach prioritizing mesenteric revascularization before central aortic repair in AAD complicated by visceral malperfusion. By first addressing end-organ ischemia, we potentially mitigated the risk of irreversible bowel necrosis while enabling subsequent central aortic repair. Our experience adds to the growing body of evidence supporting individualized, pathophysiology-guided treatment strategies for this challenging clinical scenario.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12179782/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0136\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0136","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/18 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Successful Emergency Stenting of a Visceral Branch Prior to Central Aortic Repair in Type A Aortic Dissection with Mesenteric Malperfusion: A Case Report.
Introduction: Stanford Type A acute aortic dissection (AAD) complicated by mesenteric malperfusion has a mortality rate exceeding 60%. Conventional immediate central aortic repair may be inadequate in such complex cases. Emerging evidence suggests that a staged approach may improve outcomes.
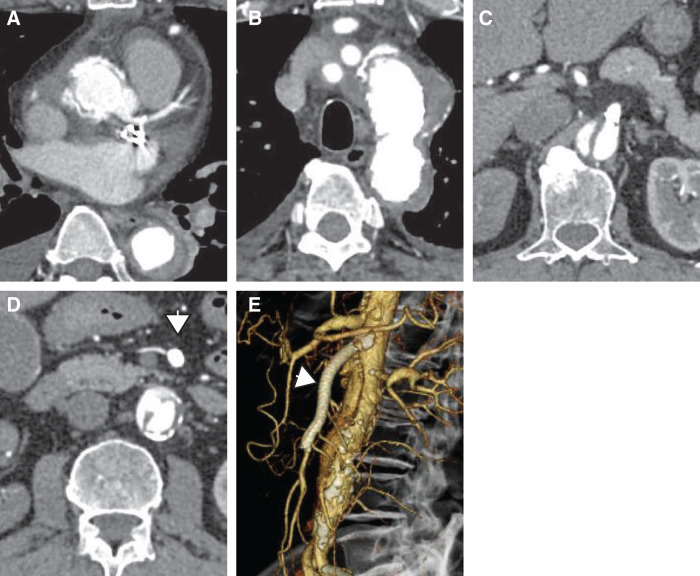
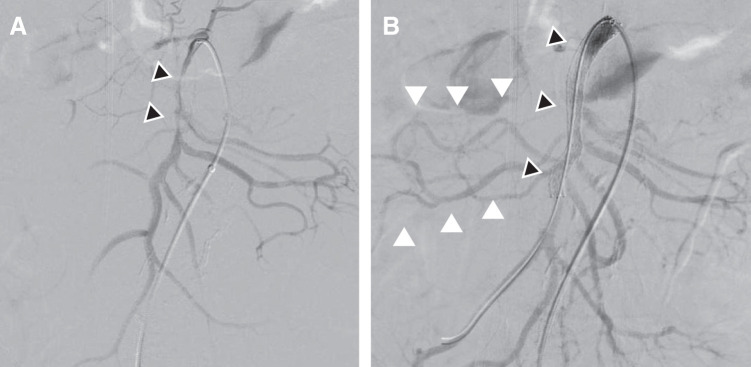
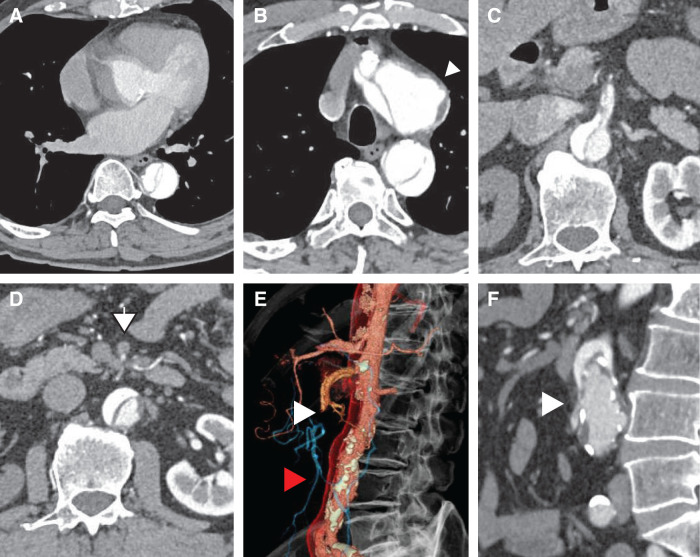
Case presentation: A 71-year-old male presented with acute chest pain and was diagnosed with Stanford Type A AAD extending to the abdominal aorta, with superior mesenteric artery (SMA) dissection leading to intestinal ischemia. To restore intestinal perfusion, emergency endovascular SMA stenting was performed as the initial intervention, followed by ascending aorta and total arch replacement using the frozen elephant trunk technique 12 hours later. The patient recovered without complications and was discharged ambulatory on postoperative day 20.
Conclusions: This case highlights the efficacy of a staged approach prioritizing mesenteric revascularization before central aortic repair in AAD complicated by visceral malperfusion. By first addressing end-organ ischemia, we potentially mitigated the risk of irreversible bowel necrosis while enabling subsequent central aortic repair. Our experience adds to the growing body of evidence supporting individualized, pathophysiology-guided treatment strategies for this challenging clinical scenario.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


