Erryk S Katayama, Sidharth Iyer, Selamawit Woldesenbet, Zayed Rashid, Mujtaba Khalil, Kristen M Carpenter, Timothy M Pawlik
{"title":"抗抑郁药对腹部肿瘤合并抑郁症患者手术结果的影响。","authors":"Erryk S Katayama, Sidharth Iyer, Selamawit Woldesenbet, Zayed Rashid, Mujtaba Khalil, Kristen M Carpenter, Timothy M Pawlik","doi":"10.1002/pon.70210","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Depression is commonly linked to cancer and may negatively impact patient outcomes; however, the influence of antidepressants on surgical outcomes remains unclear. We sought to evaluate the role of antidepressants among patients with gastrointestinal cancer and comorbid depression undergoing surgical resection.</p><p><strong>Methods: </strong>Patients diagnosed with hepatobiliary, pancreatic, and colorectal cancers (2008-2019) were identified within SEER-Medicare. Comorbid depression, within 12 months before or after a cancer diagnosis, and antidepressant prescriptions were assessed. An \"ideal\" postoperative textbook outcome required no complications, prolonged stay, 90-day readmission, or 90-day mortality. Hospitalization and post-discharge expenditures were also assessed.</p><p><strong>Results: </strong>Among 32,726 cancer patients (hepatobiliary: 2313, 7%; pancreatic: 2583, 8%; colorectal: 27,830, 85%), 1731 (5.3%) had documented depression (478 treated vs. 1253 untreated with antidepressant medications). Patients were more likely to receive treatment for depression if they were female (treated: 71% vs. untreated: 68%), White (treated: 88% vs. untreated: 80%), and had lower comorbidity burden (treated: 65% vs. untreated: 54%) (all p < 0.001). Patients with depression, both treated and untreated, had worse postoperative outcomes. Preoperative treatment with antidepressants decreased the effect of depression on adverse outcomes as patients with untreated depression were more likely to experience complications, prolonged stay, readmission, and mortality (all p < 0.001). Patients with untreated depression incurred higher in-hospital and 90-day post-discharge expenditures (no depression: $17,551; treated: $22,086 [7.3% increase]; untreated: $24,897 [10.2% increase]; p < 0.001).</p><p><strong>Conclusions: </strong>Depression reduced the likelihood to achieve optimal postoperative outcomes, yet antidepressant treatment preoperatively mitigated the size of these effects. Screening for depression and initiating appropriate therapy may enhance outcomes.</p>","PeriodicalId":20779,"journal":{"name":"Psycho‐Oncology","volume":"34 6","pages":"e70210"},"PeriodicalIF":3.5000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185974/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Antidepressants on Surgical Outcomes Among Patients With Abdominal Cancer and Comorbid Depression.\",\"authors\":\"Erryk S Katayama, Sidharth Iyer, Selamawit Woldesenbet, Zayed Rashid, Mujtaba Khalil, Kristen M Carpenter, Timothy M Pawlik\",\"doi\":\"10.1002/pon.70210\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Depression is commonly linked to cancer and may negatively impact patient outcomes; however, the influence of antidepressants on surgical outcomes remains unclear. We sought to evaluate the role of antidepressants among patients with gastrointestinal cancer and comorbid depression undergoing surgical resection.</p><p><strong>Methods: </strong>Patients diagnosed with hepatobiliary, pancreatic, and colorectal cancers (2008-2019) were identified within SEER-Medicare. Comorbid depression, within 12 months before or after a cancer diagnosis, and antidepressant prescriptions were assessed. An \\\"ideal\\\" postoperative textbook outcome required no complications, prolonged stay, 90-day readmission, or 90-day mortality. Hospitalization and post-discharge expenditures were also assessed.</p><p><strong>Results: </strong>Among 32,726 cancer patients (hepatobiliary: 2313, 7%; pancreatic: 2583, 8%; colorectal: 27,830, 85%), 1731 (5.3%) had documented depression (478 treated vs. 1253 untreated with antidepressant medications). Patients were more likely to receive treatment for depression if they were female (treated: 71% vs. untreated: 68%), White (treated: 88% vs. untreated: 80%), and had lower comorbidity burden (treated: 65% vs. untreated: 54%) (all p < 0.001). Patients with depression, both treated and untreated, had worse postoperative outcomes. Preoperative treatment with antidepressants decreased the effect of depression on adverse outcomes as patients with untreated depression were more likely to experience complications, prolonged stay, readmission, and mortality (all p < 0.001). Patients with untreated depression incurred higher in-hospital and 90-day post-discharge expenditures (no depression: $17,551; treated: $22,086 [7.3% increase]; untreated: $24,897 [10.2% increase]; p < 0.001).</p><p><strong>Conclusions: </strong>Depression reduced the likelihood to achieve optimal postoperative outcomes, yet antidepressant treatment preoperatively mitigated the size of these effects. Screening for depression and initiating appropriate therapy may enhance outcomes.</p>\",\"PeriodicalId\":20779,\"journal\":{\"name\":\"Psycho‐Oncology\",\"volume\":\"34 6\",\"pages\":\"e70210\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12185974/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Psycho‐Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/pon.70210\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psycho‐Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pon.70210","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
The Impact of Antidepressants on Surgical Outcomes Among Patients With Abdominal Cancer and Comorbid Depression.
Objective: Depression is commonly linked to cancer and may negatively impact patient outcomes; however, the influence of antidepressants on surgical outcomes remains unclear. We sought to evaluate the role of antidepressants among patients with gastrointestinal cancer and comorbid depression undergoing surgical resection.
Methods: Patients diagnosed with hepatobiliary, pancreatic, and colorectal cancers (2008-2019) were identified within SEER-Medicare. Comorbid depression, within 12 months before or after a cancer diagnosis, and antidepressant prescriptions were assessed. An "ideal" postoperative textbook outcome required no complications, prolonged stay, 90-day readmission, or 90-day mortality. Hospitalization and post-discharge expenditures were also assessed.
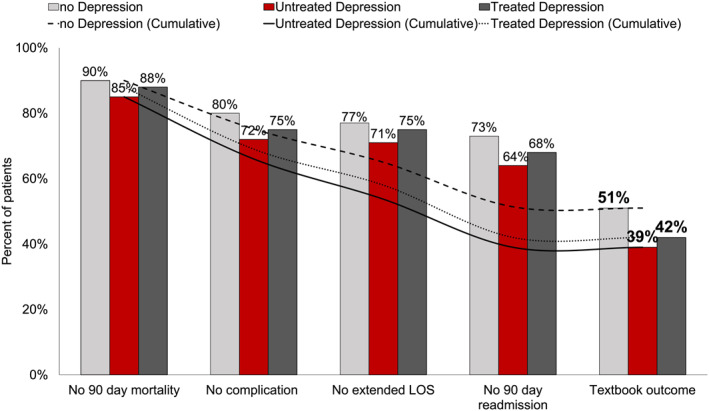
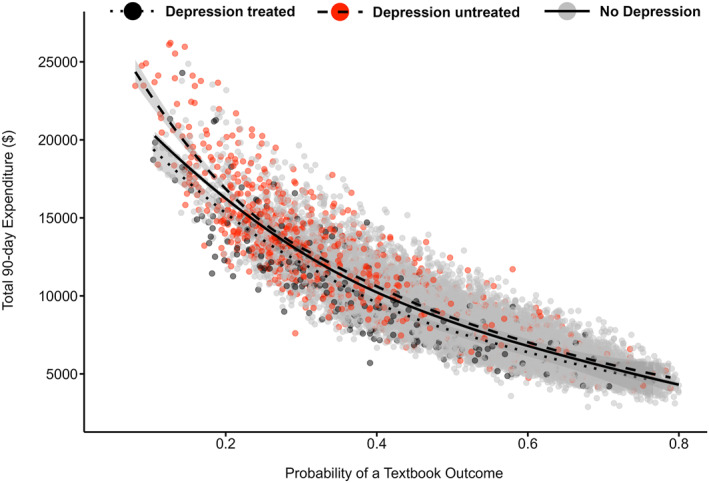
Results: Among 32,726 cancer patients (hepatobiliary: 2313, 7%; pancreatic: 2583, 8%; colorectal: 27,830, 85%), 1731 (5.3%) had documented depression (478 treated vs. 1253 untreated with antidepressant medications). Patients were more likely to receive treatment for depression if they were female (treated: 71% vs. untreated: 68%), White (treated: 88% vs. untreated: 80%), and had lower comorbidity burden (treated: 65% vs. untreated: 54%) (all p < 0.001). Patients with depression, both treated and untreated, had worse postoperative outcomes. Preoperative treatment with antidepressants decreased the effect of depression on adverse outcomes as patients with untreated depression were more likely to experience complications, prolonged stay, readmission, and mortality (all p < 0.001). Patients with untreated depression incurred higher in-hospital and 90-day post-discharge expenditures (no depression: $17,551; treated: $22,086 [7.3% increase]; untreated: $24,897 [10.2% increase]; p < 0.001).
Conclusions: Depression reduced the likelihood to achieve optimal postoperative outcomes, yet antidepressant treatment preoperatively mitigated the size of these effects. Screening for depression and initiating appropriate therapy may enhance outcomes.
期刊介绍:
Psycho-Oncology is concerned with the psychological, social, behavioral, and ethical aspects of cancer. This subspeciality addresses the two major psychological dimensions of cancer: the psychological responses of patients to cancer at all stages of the disease, and that of their families and caretakers; and the psychological, behavioral and social factors that may influence the disease process. Psycho-oncology is an area of multi-disciplinary interest and has boundaries with the major specialities in oncology: the clinical disciplines (surgery, medicine, pediatrics, radiotherapy), epidemiology, immunology, endocrinology, biology, pathology, bioethics, palliative care, rehabilitation medicine, clinical trials research and decision making, as well as psychiatry and psychology.
This international journal is published twelve times a year and will consider contributions to research of clinical and theoretical interest. Topics covered are wide-ranging and relate to the psychosocial aspects of cancer and AIDS-related tumors, including: epidemiology, quality of life, palliative and supportive care, psychiatry, psychology, sociology, social work, nursing and educational issues.
Special reviews are offered from time to time. There is a section reviewing recently published books. A society news section is available for the dissemination of information relating to meetings, conferences and other society-related topics. Summary proceedings of important national and international symposia falling within the aims of the journal are presented.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


