{"title":"皮下脂肪面积可作为肺癌肺叶切除术后引流量的预测指标。","authors":"Jie Xu, Shuai Yuan, Xiaopeng An, Jie Dong","doi":"10.1111/1759-7714.70114","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Currently, no uniform standard exists for the maximum drainage volume permitting chest tube removal following lobectomy in lung cancer patients, and limited research has explored factors influencing postoperative drainage. This study aimed to investigate the relationship between subcutaneous fat area (SFA) and postoperative drainage volume.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 509 lung cancer patients who underwent video-assisted thoracoscopic lobectomy. Clinical characteristics, postoperative outcomes (length of stay, hospitalization expenses), blood parameters, chest tube duration, 3-day postoperative drainage volume, and SFA were recorded. Predictive factors for drainage volume were identified using univariate and multivariate logistic regression analyses. SFA was measured at the level of the 12th thoracic vertebra cross-section using preoperative CT imaging.</p><p><strong>Results: </strong>The analysis revealed significant positive correlations between chest tube duration and both length of stay (p < 0.001) and hospitalization expenses (p < 0.001). Chest tube duration (< 3 vs. ≥ 3 days) was primarily determined by 3-day postoperative drainage volume (574 ± 252 vs. 885 ± 362 mL; p < 0.001). Univariate analysis demonstrated that 3-day postoperative drainage volume correlated with age (p < 0.001), gender (p = 0.002), pathological type (p < 0.001), diabetes (p = 0.026), hypertension (p = 0.011), and SFA (p < 0.001). Multivariate logistic regression confirmed that age ≥ 65 years (p = 0.016), small cell lung cancer (SCLC; p = 0.022), and SFA ≥ 100 cm<sup>2</sup> (p = 0.005) were independently associated with postoperative drainage volume ≥ 650 mL.</p><p><strong>Conclusions: </strong>SFA significantly correlated with 3-day postoperative drainage volume and may serve as a predictor for drainage volume following lobectomy in lung cancer patients. This association highlights its utility in guiding chest tube removal timing and potentially reducing the risk of pleural effusion recurrence.</p>","PeriodicalId":23338,"journal":{"name":"Thoracic Cancer","volume":"16 12","pages":"e70114"},"PeriodicalIF":2.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12181634/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subcutaneous Fat Area Can Be as a Predictors of Drainage Volume After Lobectomy for Lung Cancer.\",\"authors\":\"Jie Xu, Shuai Yuan, Xiaopeng An, Jie Dong\",\"doi\":\"10.1111/1759-7714.70114\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Currently, no uniform standard exists for the maximum drainage volume permitting chest tube removal following lobectomy in lung cancer patients, and limited research has explored factors influencing postoperative drainage. This study aimed to investigate the relationship between subcutaneous fat area (SFA) and postoperative drainage volume.</p><p><strong>Methods: </strong>We conducted a retrospective analysis of 509 lung cancer patients who underwent video-assisted thoracoscopic lobectomy. Clinical characteristics, postoperative outcomes (length of stay, hospitalization expenses), blood parameters, chest tube duration, 3-day postoperative drainage volume, and SFA were recorded. Predictive factors for drainage volume were identified using univariate and multivariate logistic regression analyses. SFA was measured at the level of the 12th thoracic vertebra cross-section using preoperative CT imaging.</p><p><strong>Results: </strong>The analysis revealed significant positive correlations between chest tube duration and both length of stay (p < 0.001) and hospitalization expenses (p < 0.001). Chest tube duration (< 3 vs. ≥ 3 days) was primarily determined by 3-day postoperative drainage volume (574 ± 252 vs. 885 ± 362 mL; p < 0.001). Univariate analysis demonstrated that 3-day postoperative drainage volume correlated with age (p < 0.001), gender (p = 0.002), pathological type (p < 0.001), diabetes (p = 0.026), hypertension (p = 0.011), and SFA (p < 0.001). Multivariate logistic regression confirmed that age ≥ 65 years (p = 0.016), small cell lung cancer (SCLC; p = 0.022), and SFA ≥ 100 cm<sup>2</sup> (p = 0.005) were independently associated with postoperative drainage volume ≥ 650 mL.</p><p><strong>Conclusions: </strong>SFA significantly correlated with 3-day postoperative drainage volume and may serve as a predictor for drainage volume following lobectomy in lung cancer patients. This association highlights its utility in guiding chest tube removal timing and potentially reducing the risk of pleural effusion recurrence.</p>\",\"PeriodicalId\":23338,\"journal\":{\"name\":\"Thoracic Cancer\",\"volume\":\"16 12\",\"pages\":\"e70114\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12181634/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thoracic Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/1759-7714.70114\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thoracic Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/1759-7714.70114","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Subcutaneous Fat Area Can Be as a Predictors of Drainage Volume After Lobectomy for Lung Cancer.
Objective: Currently, no uniform standard exists for the maximum drainage volume permitting chest tube removal following lobectomy in lung cancer patients, and limited research has explored factors influencing postoperative drainage. This study aimed to investigate the relationship between subcutaneous fat area (SFA) and postoperative drainage volume.
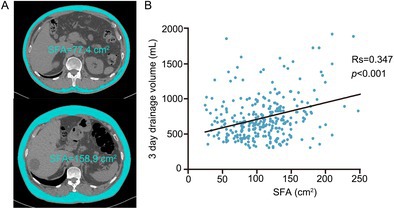
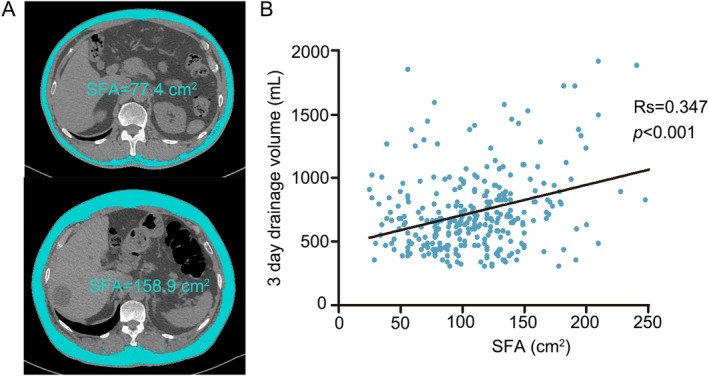
Methods: We conducted a retrospective analysis of 509 lung cancer patients who underwent video-assisted thoracoscopic lobectomy. Clinical characteristics, postoperative outcomes (length of stay, hospitalization expenses), blood parameters, chest tube duration, 3-day postoperative drainage volume, and SFA were recorded. Predictive factors for drainage volume were identified using univariate and multivariate logistic regression analyses. SFA was measured at the level of the 12th thoracic vertebra cross-section using preoperative CT imaging.
Results: The analysis revealed significant positive correlations between chest tube duration and both length of stay (p < 0.001) and hospitalization expenses (p < 0.001). Chest tube duration (< 3 vs. ≥ 3 days) was primarily determined by 3-day postoperative drainage volume (574 ± 252 vs. 885 ± 362 mL; p < 0.001). Univariate analysis demonstrated that 3-day postoperative drainage volume correlated with age (p < 0.001), gender (p = 0.002), pathological type (p < 0.001), diabetes (p = 0.026), hypertension (p = 0.011), and SFA (p < 0.001). Multivariate logistic regression confirmed that age ≥ 65 years (p = 0.016), small cell lung cancer (SCLC; p = 0.022), and SFA ≥ 100 cm2 (p = 0.005) were independently associated with postoperative drainage volume ≥ 650 mL.
Conclusions: SFA significantly correlated with 3-day postoperative drainage volume and may serve as a predictor for drainage volume following lobectomy in lung cancer patients. This association highlights its utility in guiding chest tube removal timing and potentially reducing the risk of pleural effusion recurrence.
期刊介绍:
Thoracic Cancer aims to facilitate international collaboration and exchange of comprehensive and cutting-edge information on basic, translational, and applied clinical research in lung cancer, esophageal cancer, mediastinal cancer, breast cancer and other thoracic malignancies. Prevention, treatment and research relevant to Asia-Pacific is a focus area, but submissions from all regions are welcomed. The editors encourage contributions relevant to prevention, general thoracic surgery, medical oncology, radiology, radiation medicine, pathology, basic cancer research, as well as epidemiological and translational studies in thoracic cancer. Thoracic Cancer is the official publication of the Chinese Society of Lung Cancer, International Chinese Society of Thoracic Surgery and is endorsed by the Korean Association for the Study of Lung Cancer and the Hong Kong Cancer Therapy Society.
The Journal publishes a range of article types including: Editorials, Invited Reviews, Mini Reviews, Original Articles, Clinical Guidelines, Technological Notes, Imaging in thoracic cancer, Meeting Reports, Case Reports, Letters to the Editor, Commentaries, and Brief Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


