Sao Trung Nguyen, Van-Anh Nguyen Hoang, Vu Nguyen Trieu, Thanh Huyen Pham, Thi Cuc Dinh, Dinh Hoang Pham, Ngoc Nguyen, Dao Nguyen Vinh, Thanh Thuy Thi Do, Duy Sinh Nguyen, Hoai-Nghia Nguyen, Hoa Giang, Lan N Tu
{"title":"循环肿瘤DNA的个性化突变跟踪预测高危早期乳腺癌患者的复发。","authors":"Sao Trung Nguyen, Van-Anh Nguyen Hoang, Vu Nguyen Trieu, Thanh Huyen Pham, Thi Cuc Dinh, Dinh Hoang Pham, Ngoc Nguyen, Dao Nguyen Vinh, Thanh Thuy Thi Do, Duy Sinh Nguyen, Hoai-Nghia Nguyen, Hoa Giang, Lan N Tu","doi":"10.1038/s41523-025-00778-z","DOIUrl":null,"url":null,"abstract":"<p><p>The clinical utilization of circulating tumor DNA (ctDNA) in breast cancer (BC) management is not well-defined. In this prospective study, 168 patients with early-stage BC were recruited, serial blood samples were collected before and after surgery. Tumor-informed ctDNA testing was performed, which sequenced tumors for 95 genes followed by bespoke mPCR to track 1-9 mutations in the plasma. ctDNA was detected before surgery in 14.6%, 40.0%, 83.8%, and 80.0% of HR+ low-risk, HR+ high-risk, HR-HER2+ and HR-HER2- patients, respectively. Pre-operative ctDNA positivity was significantly associated with decreased disease-free survival (DFS) (adjusted HR = 3.09, 95% CI 2.65-80.0, p = 0.001). After a median 26.6-month follow-up, 11 patients relapsed, and ctDNA at landmark time point 2-4 weeks after surgery was detected in 50.0% (5/10) of cases. Landmark ctDNA clearance was associated with significantly longer DFS (p = 0.0009) and positive ctDNA persistence after adjuvant therapy occurred in 36.4% (4/11) of stage-III patients. During surveillance, ctDNA detection had 90.9% sensitivity and 98.8% specificity to predict recurrence, and median lead time of 9.7 months. Patients with detected ctDNA had shorter DFS than those with undetectable ctDNA (adjusted HR = 207.05, 95% CI 41.38- > 1000, p = 0.001). Therefore, ctDNA status both before and after surgery could help stratify recurrence risk for BC patients.</p>","PeriodicalId":19247,"journal":{"name":"NPJ Breast Cancer","volume":"11 1","pages":"58"},"PeriodicalIF":7.6000,"publicationDate":"2025-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12181414/pdf/","citationCount":"0","resultStr":"{\"title\":\"Personalized mutation tracking in circulating-tumor DNA predicts recurrence in patients with high-risk early breast cancer.\",\"authors\":\"Sao Trung Nguyen, Van-Anh Nguyen Hoang, Vu Nguyen Trieu, Thanh Huyen Pham, Thi Cuc Dinh, Dinh Hoang Pham, Ngoc Nguyen, Dao Nguyen Vinh, Thanh Thuy Thi Do, Duy Sinh Nguyen, Hoai-Nghia Nguyen, Hoa Giang, Lan N Tu\",\"doi\":\"10.1038/s41523-025-00778-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The clinical utilization of circulating tumor DNA (ctDNA) in breast cancer (BC) management is not well-defined. In this prospective study, 168 patients with early-stage BC were recruited, serial blood samples were collected before and after surgery. Tumor-informed ctDNA testing was performed, which sequenced tumors for 95 genes followed by bespoke mPCR to track 1-9 mutations in the plasma. ctDNA was detected before surgery in 14.6%, 40.0%, 83.8%, and 80.0% of HR+ low-risk, HR+ high-risk, HR-HER2+ and HR-HER2- patients, respectively. Pre-operative ctDNA positivity was significantly associated with decreased disease-free survival (DFS) (adjusted HR = 3.09, 95% CI 2.65-80.0, p = 0.001). After a median 26.6-month follow-up, 11 patients relapsed, and ctDNA at landmark time point 2-4 weeks after surgery was detected in 50.0% (5/10) of cases. Landmark ctDNA clearance was associated with significantly longer DFS (p = 0.0009) and positive ctDNA persistence after adjuvant therapy occurred in 36.4% (4/11) of stage-III patients. During surveillance, ctDNA detection had 90.9% sensitivity and 98.8% specificity to predict recurrence, and median lead time of 9.7 months. Patients with detected ctDNA had shorter DFS than those with undetectable ctDNA (adjusted HR = 207.05, 95% CI 41.38- > 1000, p = 0.001). Therefore, ctDNA status both before and after surgery could help stratify recurrence risk for BC patients.</p>\",\"PeriodicalId\":19247,\"journal\":{\"name\":\"NPJ Breast Cancer\",\"volume\":\"11 1\",\"pages\":\"58\"},\"PeriodicalIF\":7.6000,\"publicationDate\":\"2025-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12181414/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Breast Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41523-025-00778-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Breast Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41523-025-00778-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
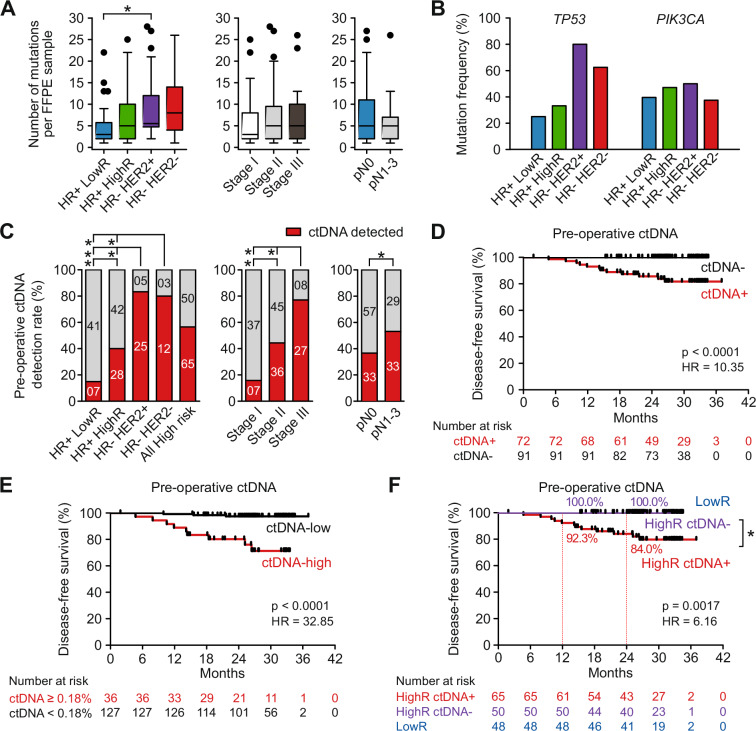
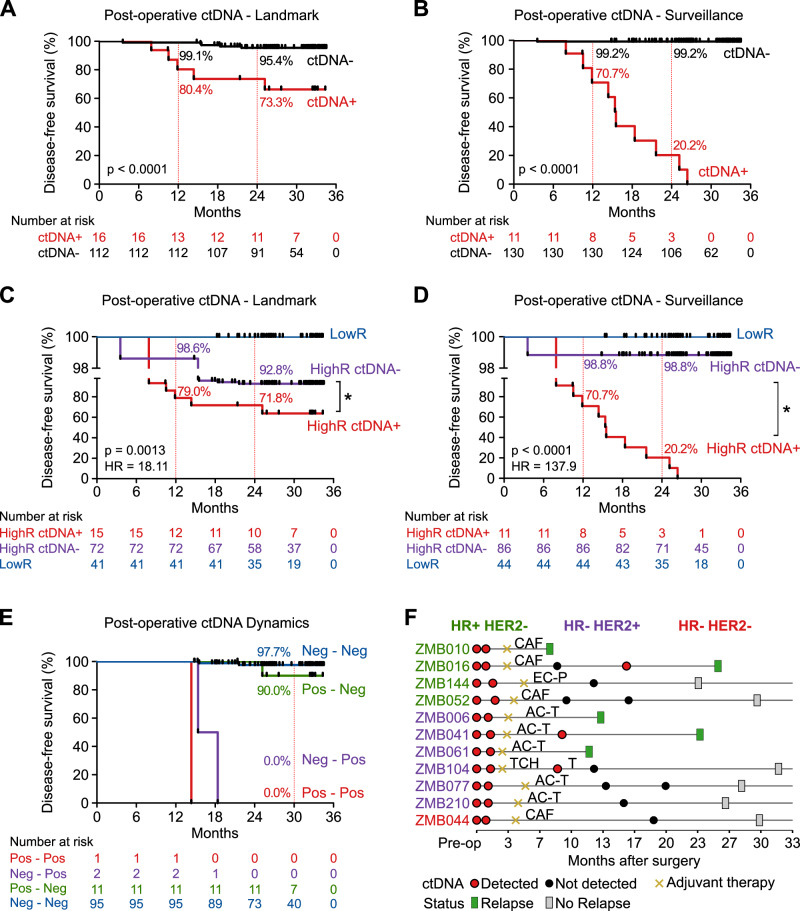
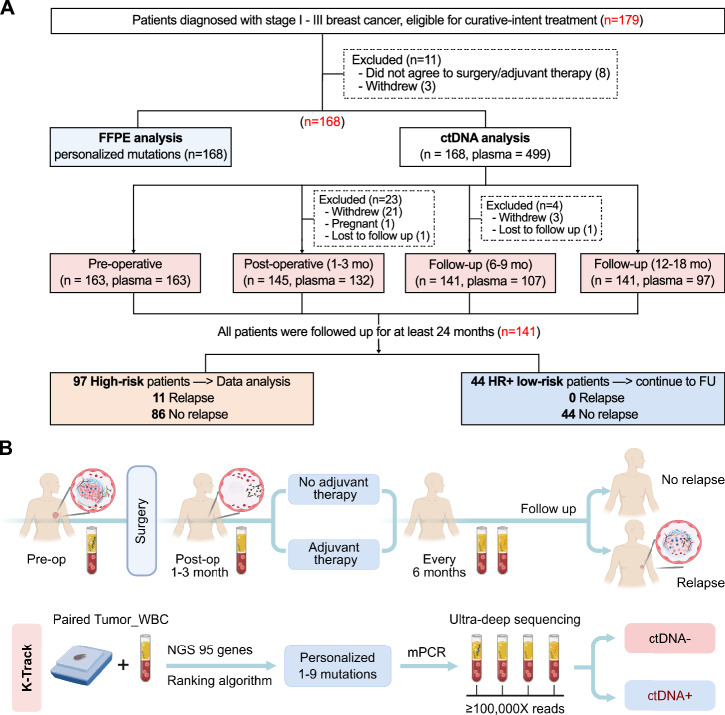
循环肿瘤DNA (ctDNA)在乳腺癌(BC)治疗中的临床应用尚不明确。在这项前瞻性研究中,招募了168例早期BC患者,在术前和术后收集了连续的血液样本。研究人员对肿瘤进行了ctDNA检测,对95个基因进行了肿瘤测序,然后使用定制的mPCR来追踪血浆中1-9个突变。术前检测ctDNA的HR+低危、HR+高危、HR- her2 +、HR- her2 -患者分别为14.6%、40.0%、83.8%、80.0%。术前ctDNA阳性与无病生存率(DFS)降低显著相关(调整后HR = 3.09, 95% CI 2.65-80.0, p = 0.001)。中位随访26.6个月后,11例患者复发,50.0%(5/10)的病例在术后2-4周的标志性时间点检测到ctDNA。里程碑式的ctDNA清除与更长的DFS相关(p = 0.0009),辅助治疗后,36.4%(4/11)的iii期患者的ctDNA持续呈阳性。在监测期间,ctDNA检测预测复发的敏感性为90.9%,特异性为98.8%,中位预诊时间为9.7个月。检测到ctDNA的患者比未检测到ctDNA的患者的DFS更短(校正后HR = 207.05, 95% CI 41.38- bbb1000, p = 0.001)。因此,术前和术后的ctDNA状态可以帮助对BC患者的复发风险进行分层。
Personalized mutation tracking in circulating-tumor DNA predicts recurrence in patients with high-risk early breast cancer.
The clinical utilization of circulating tumor DNA (ctDNA) in breast cancer (BC) management is not well-defined. In this prospective study, 168 patients with early-stage BC were recruited, serial blood samples were collected before and after surgery. Tumor-informed ctDNA testing was performed, which sequenced tumors for 95 genes followed by bespoke mPCR to track 1-9 mutations in the plasma. ctDNA was detected before surgery in 14.6%, 40.0%, 83.8%, and 80.0% of HR+ low-risk, HR+ high-risk, HR-HER2+ and HR-HER2- patients, respectively. Pre-operative ctDNA positivity was significantly associated with decreased disease-free survival (DFS) (adjusted HR = 3.09, 95% CI 2.65-80.0, p = 0.001). After a median 26.6-month follow-up, 11 patients relapsed, and ctDNA at landmark time point 2-4 weeks after surgery was detected in 50.0% (5/10) of cases. Landmark ctDNA clearance was associated with significantly longer DFS (p = 0.0009) and positive ctDNA persistence after adjuvant therapy occurred in 36.4% (4/11) of stage-III patients. During surveillance, ctDNA detection had 90.9% sensitivity and 98.8% specificity to predict recurrence, and median lead time of 9.7 months. Patients with detected ctDNA had shorter DFS than those with undetectable ctDNA (adjusted HR = 207.05, 95% CI 41.38- > 1000, p = 0.001). Therefore, ctDNA status both before and after surgery could help stratify recurrence risk for BC patients.
期刊介绍:
npj Breast Cancer publishes original research articles, reviews, brief correspondence, meeting reports, editorial summaries and hypothesis generating observations which could be unexplained or preliminary findings from experiments, novel ideas, or the framing of new questions that need to be solved. Featured topics of the journal include imaging, immunotherapy, molecular classification of disease, mechanism-based therapies largely targeting signal transduction pathways, carcinogenesis including hereditary susceptibility and molecular epidemiology, survivorship issues including long-term toxicities of treatment and secondary neoplasm occurrence, the biophysics of cancer, mechanisms of metastasis and their perturbation, and studies of the tumor microenvironment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


