Hye Sung Kim, Wongi Woo, Young-Geun Choi, Ankit Bharat, Young Kwang Chae
{"title":"实体器官移植中移植排斥反应与移植后恶性肿瘤之间的新联系。","authors":"Hye Sung Kim, Wongi Woo, Young-Geun Choi, Ankit Bharat, Young Kwang Chae","doi":"10.5500/wjt.v15.i2.102384","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Advancements in immunosuppressive therapies have improved graft survival by enhancing graft tolerance and preventing organ rejection. However, the risk of malignancy associated with prolonged immunosuppression remains a concern, as it can adversely affect recipients' quality of life and survival. While the link between immunosuppression and increased cancer risk is well-documented, the specific interactions between graft rejection and post-transplant malignancy (PTM) remain poorly understood. Addressing this knowledge gap is crucial for devising immunosuppressive strategies that balance rejection prevention with cancer risk reduction.</p><p><strong>Aim: </strong>To investigate whether immunosuppression in PTM reduces rejection risk, while immune activation during rejection protects against malignancy.</p><p><strong>Methods: </strong>We analyzed data from the United Network for Organ Sharing's Organ Procurement and Transplantation Network database (1987-2023) on adult, first-time, single-organ transplant recipients with no prior history of malignancy (in donors or recipients). Landmark analyses at 1, 2, 3, 5, 10, 15, and 20 years post-transplant, Kaplan-Meier analyses, and time-dependent Cox proportional hazards regression models, each incorporating the temporal dimension of outcomes, assessed the association between rejection-induced graft failure (RGF) and PTM. Multivariate models were adjusted for clinical and immunological factors, including immunosuppression regimens.</p><p><strong>Results: </strong>The cohort included 579905 recipients (kidney: 386878; liver: 108390; heart: 45046; lung: 37643; pancreas: 1948) with a mean follow-up of 7.3 years and a median age of 50.6 ± 13.2 years. RGF was associated with a reduction in PTM risk across all time points [hazard ratio (HR) = 0.07-0.20, <i>P</i> < 0.001], even after excluding mortality cases. Kidney transplant recipients exhibited the most pronounced reduction (HR = 0.22, <i>P</i> < 0.001). Conversely, among recipients with PTM, RGF risk decreased across all time points up to 15 years after excluding mortality cases (HR = 0.49-0.80, <i>P</i> < 0.001). This risk reduction was observed in kidney, liver, heart, and lung transplants (HRs = 0.90, 0.21, 0.21, and 0.18, respectively; <i>P</i> < 0.001) but not in pancreas transplants.</p><p><strong>Conclusion: </strong>RGF reduces PTM risk, particularly in kidney transplants, while PTM decreases RGF risk in kidney, liver, heart, and lung transplants.</p>","PeriodicalId":65557,"journal":{"name":"世界移植杂志","volume":"15 2","pages":"102384"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11886299/pdf/","citationCount":"0","resultStr":"{\"title\":\"Novel association between graft rejection and post-transplant malignancy in solid organ transplantation.\",\"authors\":\"Hye Sung Kim, Wongi Woo, Young-Geun Choi, Ankit Bharat, Young Kwang Chae\",\"doi\":\"10.5500/wjt.v15.i2.102384\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Advancements in immunosuppressive therapies have improved graft survival by enhancing graft tolerance and preventing organ rejection. However, the risk of malignancy associated with prolonged immunosuppression remains a concern, as it can adversely affect recipients' quality of life and survival. While the link between immunosuppression and increased cancer risk is well-documented, the specific interactions between graft rejection and post-transplant malignancy (PTM) remain poorly understood. Addressing this knowledge gap is crucial for devising immunosuppressive strategies that balance rejection prevention with cancer risk reduction.</p><p><strong>Aim: </strong>To investigate whether immunosuppression in PTM reduces rejection risk, while immune activation during rejection protects against malignancy.</p><p><strong>Methods: </strong>We analyzed data from the United Network for Organ Sharing's Organ Procurement and Transplantation Network database (1987-2023) on adult, first-time, single-organ transplant recipients with no prior history of malignancy (in donors or recipients). Landmark analyses at 1, 2, 3, 5, 10, 15, and 20 years post-transplant, Kaplan-Meier analyses, and time-dependent Cox proportional hazards regression models, each incorporating the temporal dimension of outcomes, assessed the association between rejection-induced graft failure (RGF) and PTM. Multivariate models were adjusted for clinical and immunological factors, including immunosuppression regimens.</p><p><strong>Results: </strong>The cohort included 579905 recipients (kidney: 386878; liver: 108390; heart: 45046; lung: 37643; pancreas: 1948) with a mean follow-up of 7.3 years and a median age of 50.6 ± 13.2 years. RGF was associated with a reduction in PTM risk across all time points [hazard ratio (HR) = 0.07-0.20, <i>P</i> < 0.001], even after excluding mortality cases. Kidney transplant recipients exhibited the most pronounced reduction (HR = 0.22, <i>P</i> < 0.001). Conversely, among recipients with PTM, RGF risk decreased across all time points up to 15 years after excluding mortality cases (HR = 0.49-0.80, <i>P</i> < 0.001). This risk reduction was observed in kidney, liver, heart, and lung transplants (HRs = 0.90, 0.21, 0.21, and 0.18, respectively; <i>P</i> < 0.001) but not in pancreas transplants.</p><p><strong>Conclusion: </strong>RGF reduces PTM risk, particularly in kidney transplants, while PTM decreases RGF risk in kidney, liver, heart, and lung transplants.</p>\",\"PeriodicalId\":65557,\"journal\":{\"name\":\"世界移植杂志\",\"volume\":\"15 2\",\"pages\":\"102384\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11886299/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"世界移植杂志\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.5500/wjt.v15.i2.102384\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"世界移植杂志","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5500/wjt.v15.i2.102384","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:免疫抑制疗法的进步通过增强移植物耐受性和防止器官排斥来改善移植物存活。然而,与长期免疫抑制相关的恶性肿瘤风险仍然是一个问题,因为它可能对接受者的生活质量和生存产生不利影响。虽然免疫抑制与癌症风险增加之间的联系已被充分证明,但移植排斥反应与移植后恶性肿瘤(PTM)之间的具体相互作用仍知之甚少。解决这一知识差距对于设计平衡排斥预防与降低癌症风险的免疫抑制策略至关重要。目的:探讨PTM的免疫抑制是否能降低排斥风险,而排斥过程中的免疫激活是否能预防恶性肿瘤。方法:我们分析了来自器官共享联合网络的器官获取和移植网络数据库(1987-2023)的成人、首次、无恶性肿瘤病史的单器官移植受者(供者或受者)的数据。移植后1年、2年、3年、5年、10年、15年和20年的里程碑分析、Kaplan-Meier分析和时间相关的Cox比例风险回归模型,均纳入了结果的时间维度,评估了排斥诱导的移植失败(RGF)和PTM之间的关系。根据临床和免疫因素(包括免疫抑制方案)调整多变量模型。结果:该队列包括579905名受者(肾脏:386878;肝脏:108390;心:45046;肺:37643;胰腺:1948),平均随访7.3年,中位年龄50.6±13.2岁。即使在排除死亡病例后,RGF与所有时间点PTM风险的降低相关[危险比(HR) = 0.07-0.20, P < 0.001]。肾移植受者表现出最明显的降低(HR = 0.22, P < 0.001)。相反,在PTM受者中,排除死亡病例后15年的RGF风险在所有时间点均下降(HR = 0.49-0.80, P < 0.001)。在肾脏、肝脏、心脏和肺移植中观察到这种风险降低(hr分别= 0.90、0.21、0.21和0.18;P < 0.001),但在胰腺移植中没有。结论:RGF可降低肾移植中PTM的风险,而PTM可降低肾、肝、心、肺移植中RGF的风险。
Novel association between graft rejection and post-transplant malignancy in solid organ transplantation.
Background: Advancements in immunosuppressive therapies have improved graft survival by enhancing graft tolerance and preventing organ rejection. However, the risk of malignancy associated with prolonged immunosuppression remains a concern, as it can adversely affect recipients' quality of life and survival. While the link between immunosuppression and increased cancer risk is well-documented, the specific interactions between graft rejection and post-transplant malignancy (PTM) remain poorly understood. Addressing this knowledge gap is crucial for devising immunosuppressive strategies that balance rejection prevention with cancer risk reduction.
Aim: To investigate whether immunosuppression in PTM reduces rejection risk, while immune activation during rejection protects against malignancy.
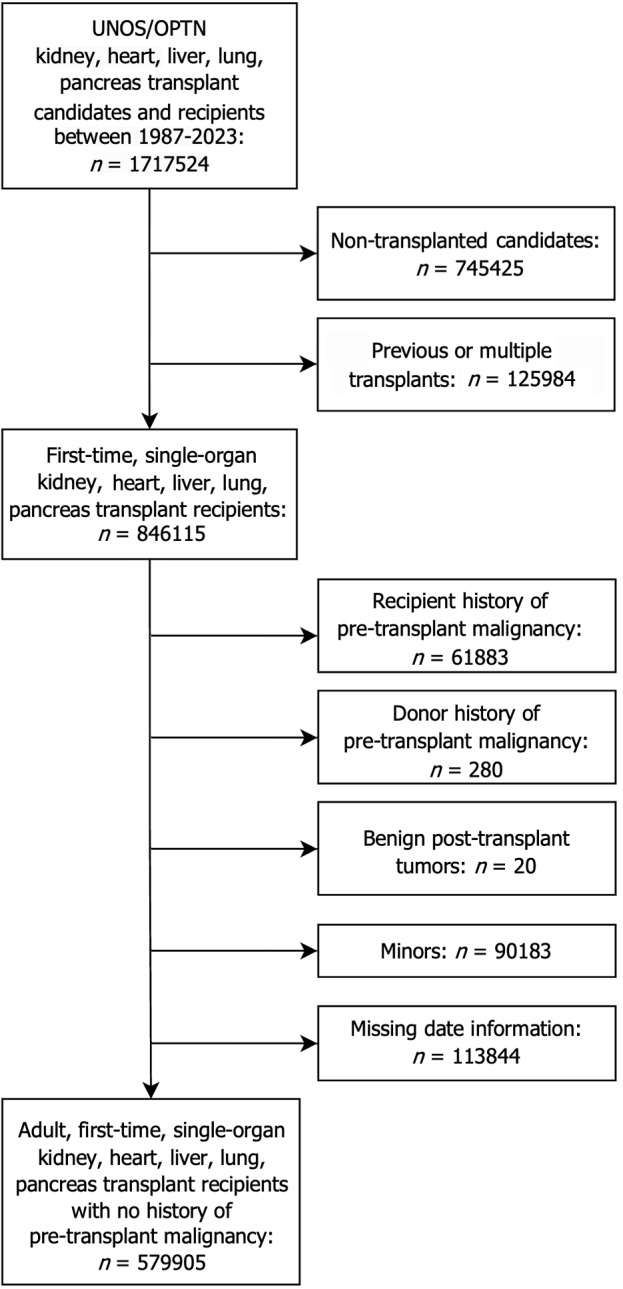
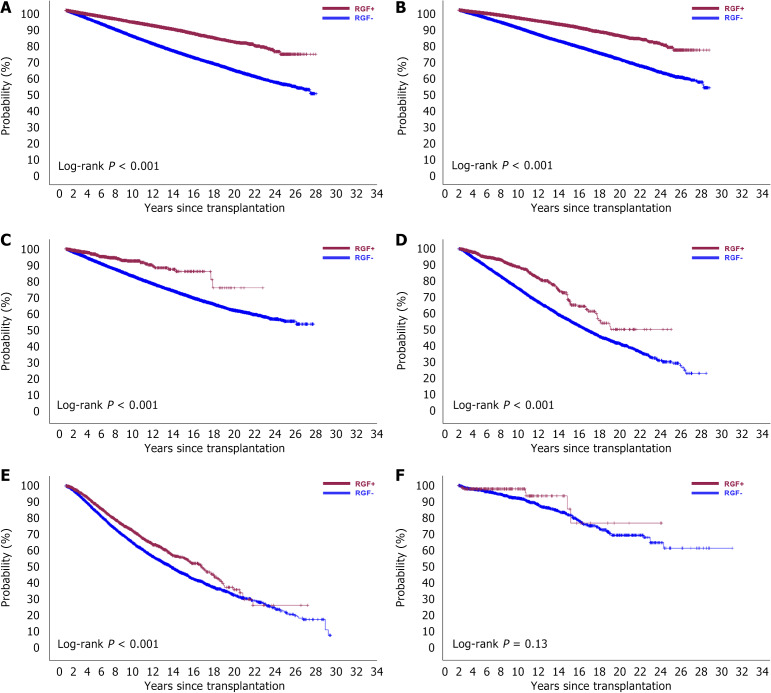
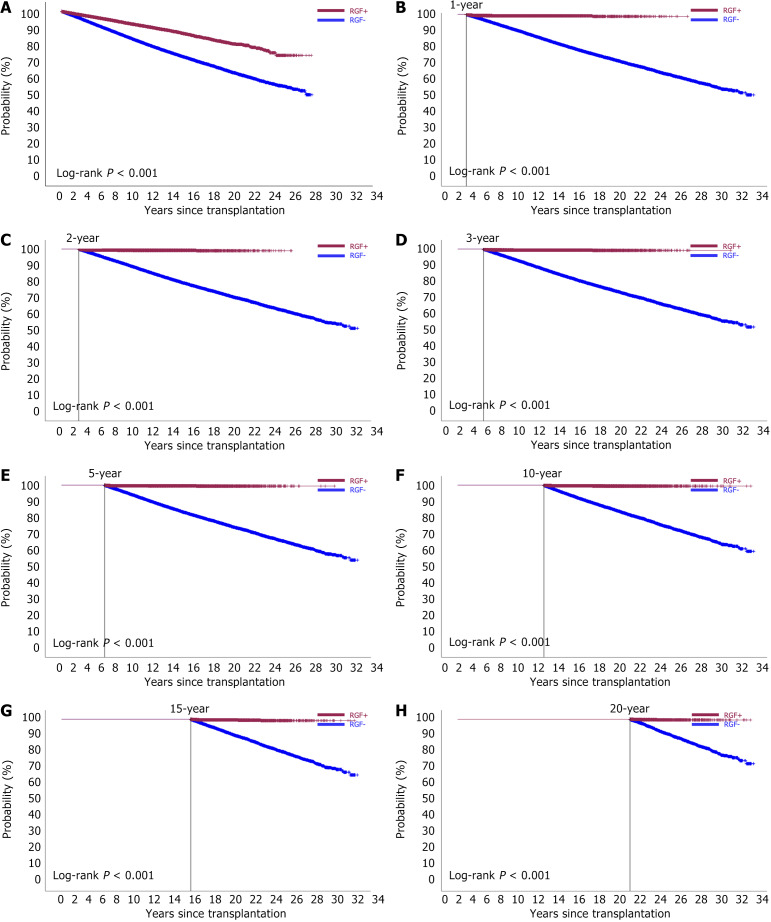
Methods: We analyzed data from the United Network for Organ Sharing's Organ Procurement and Transplantation Network database (1987-2023) on adult, first-time, single-organ transplant recipients with no prior history of malignancy (in donors or recipients). Landmark analyses at 1, 2, 3, 5, 10, 15, and 20 years post-transplant, Kaplan-Meier analyses, and time-dependent Cox proportional hazards regression models, each incorporating the temporal dimension of outcomes, assessed the association between rejection-induced graft failure (RGF) and PTM. Multivariate models were adjusted for clinical and immunological factors, including immunosuppression regimens.
Results: The cohort included 579905 recipients (kidney: 386878; liver: 108390; heart: 45046; lung: 37643; pancreas: 1948) with a mean follow-up of 7.3 years and a median age of 50.6 ± 13.2 years. RGF was associated with a reduction in PTM risk across all time points [hazard ratio (HR) = 0.07-0.20, P < 0.001], even after excluding mortality cases. Kidney transplant recipients exhibited the most pronounced reduction (HR = 0.22, P < 0.001). Conversely, among recipients with PTM, RGF risk decreased across all time points up to 15 years after excluding mortality cases (HR = 0.49-0.80, P < 0.001). This risk reduction was observed in kidney, liver, heart, and lung transplants (HRs = 0.90, 0.21, 0.21, and 0.18, respectively; P < 0.001) but not in pancreas transplants.
Conclusion: RGF reduces PTM risk, particularly in kidney transplants, while PTM decreases RGF risk in kidney, liver, heart, and lung transplants.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


