{"title":"脊髓刺激治疗腹部弥漫性内脏痛觉过敏1例报告及文献复习。","authors":"James Mamaril-Davis, Ryan Palsma, Martin Weinand","doi":"10.1159/000546229","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Spinal cord stimulation (SCS) for chronic abdominal pain is not novel. However, this has been explored only when the pain has a clear dermatomal association such as the right upper quadrant for sphincter of Oddi dysfunction or the left upper quadrant for post-traumatic splenectomy. The present report thereby discusses the utility of SCS when the visceral pain is diffusely distributed across all four quadrants of the abdomen.</p><p><strong>Case presentation: </strong>A patient in their 70s presented with a 30-year history of chronic abdominal pain diffusely located in all four quadrants. The patient had a pancreatic cyst removed via pancreaticoduodenectomy in 1991 complicated by chronic pancreatitis and visceral hyperalgesia. After failed pharmacological management and various outpatient nerve blocks and trigger point injections, the patient underwent SCS placement via five 4-contact paddle leads at the mid- to superior thoracic 7 level. At 1-month follow-up, the patient's visual analog scale score decreased from 8/10 (prior to implantation) to 0/10. The patient also discontinued his chronic opioid regimen post-SCS placement but continued duloxetine. Device settings remained the same throughout the postoperative period: pulse width of 500 microseconds (inter-burst) and 1,000 microseconds, frequency of 40 Hertz, and current of 1.7 milliamperes. At 12-month follow-up, the patient continued to report >90% pain relief at nearly the same SCS settings as the initial programming.</p><p><strong>Conclusion: </strong>SCS may be a reliable treatment option for chronic abdominal, visceral hyperalgesia when the pain is diffusely located in all 4 quadrants and without a clear dermatomal pattern.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"461-466"},"PeriodicalIF":0.6000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12176363/pdf/","citationCount":"0","resultStr":"{\"title\":\"Spinal Cord Stimulation for Diffuse Visceral Hyperalgesia in the Abdomen: A Case Report and Literature Review.\",\"authors\":\"James Mamaril-Davis, Ryan Palsma, Martin Weinand\",\"doi\":\"10.1159/000546229\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Spinal cord stimulation (SCS) for chronic abdominal pain is not novel. However, this has been explored only when the pain has a clear dermatomal association such as the right upper quadrant for sphincter of Oddi dysfunction or the left upper quadrant for post-traumatic splenectomy. The present report thereby discusses the utility of SCS when the visceral pain is diffusely distributed across all four quadrants of the abdomen.</p><p><strong>Case presentation: </strong>A patient in their 70s presented with a 30-year history of chronic abdominal pain diffusely located in all four quadrants. The patient had a pancreatic cyst removed via pancreaticoduodenectomy in 1991 complicated by chronic pancreatitis and visceral hyperalgesia. After failed pharmacological management and various outpatient nerve blocks and trigger point injections, the patient underwent SCS placement via five 4-contact paddle leads at the mid- to superior thoracic 7 level. At 1-month follow-up, the patient's visual analog scale score decreased from 8/10 (prior to implantation) to 0/10. The patient also discontinued his chronic opioid regimen post-SCS placement but continued duloxetine. Device settings remained the same throughout the postoperative period: pulse width of 500 microseconds (inter-burst) and 1,000 microseconds, frequency of 40 Hertz, and current of 1.7 milliamperes. At 12-month follow-up, the patient continued to report >90% pain relief at nearly the same SCS settings as the initial programming.</p><p><strong>Conclusion: </strong>SCS may be a reliable treatment option for chronic abdominal, visceral hyperalgesia when the pain is diffusely located in all 4 quadrants and without a clear dermatomal pattern.</p>\",\"PeriodicalId\":9614,\"journal\":{\"name\":\"Case Reports in Gastroenterology\",\"volume\":\"19 1\",\"pages\":\"461-466\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2025-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12176363/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000546229\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546229","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Spinal Cord Stimulation for Diffuse Visceral Hyperalgesia in the Abdomen: A Case Report and Literature Review.
Introduction: Spinal cord stimulation (SCS) for chronic abdominal pain is not novel. However, this has been explored only when the pain has a clear dermatomal association such as the right upper quadrant for sphincter of Oddi dysfunction or the left upper quadrant for post-traumatic splenectomy. The present report thereby discusses the utility of SCS when the visceral pain is diffusely distributed across all four quadrants of the abdomen.
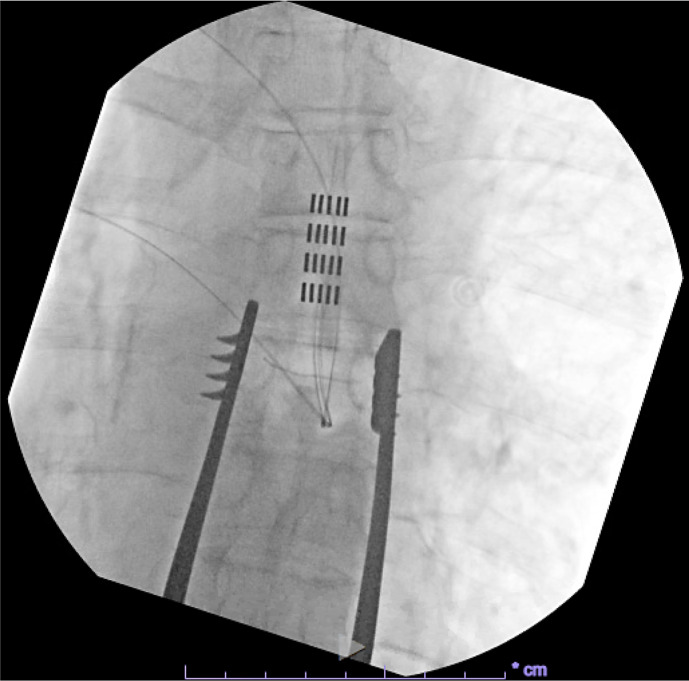
Case presentation: A patient in their 70s presented with a 30-year history of chronic abdominal pain diffusely located in all four quadrants. The patient had a pancreatic cyst removed via pancreaticoduodenectomy in 1991 complicated by chronic pancreatitis and visceral hyperalgesia. After failed pharmacological management and various outpatient nerve blocks and trigger point injections, the patient underwent SCS placement via five 4-contact paddle leads at the mid- to superior thoracic 7 level. At 1-month follow-up, the patient's visual analog scale score decreased from 8/10 (prior to implantation) to 0/10. The patient also discontinued his chronic opioid regimen post-SCS placement but continued duloxetine. Device settings remained the same throughout the postoperative period: pulse width of 500 microseconds (inter-burst) and 1,000 microseconds, frequency of 40 Hertz, and current of 1.7 milliamperes. At 12-month follow-up, the patient continued to report >90% pain relief at nearly the same SCS settings as the initial programming.
Conclusion: SCS may be a reliable treatment option for chronic abdominal, visceral hyperalgesia when the pain is diffusely located in all 4 quadrants and without a clear dermatomal pattern.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


