Matías Pécora, Piero Pastorini, Roberto Farolini, Gastón Burghi, F Javier Hurtado
{"title":"重症监护病房机械通气患者左心室收缩纵向应变:整体和腔室再现性评估。","authors":"Matías Pécora, Piero Pastorini, Roberto Farolini, Gastón Burghi, F Javier Hurtado","doi":"10.1186/s40635-025-00770-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>In the intensive care unit (ICU), left ventricular systolic function is traditionally assessed by measuring the left ventricular ejection fraction (LVEF). Recently, left ventricular global systolic longitudinal strain (SL-S) has emerged as a more sensitive marker of myocardial function in this setting. However, obtaining high-quality echocardiographic images remains a significant challenge, particularly in patients undergoing invasive mechanical ventilation (IMV), and data on the feasibility and reproducibility of these measurements in critically ill patients are limited.</p><p><strong>Objective: </strong>To assess the feasibility and reproducibility (both global and per chamber) of SL-S and LVEF (both manual and automatic) in ICU patients under IMV.</p><p><strong>Materials and methods: </strong>Thirty ICU patients receiving IMV were randomly selected. The feasibility and reproducibility of SL-S (global and per chamber) and LVEF were assessed using both manual and automatic methods. The analysis was performed using the intraclass correlation coefficient (ICC) with its 95% confidence interval (CI), and Bland-Altman analysis (BA), which reported the mean difference and limits of agreement (lower-upper limits of agreement).</p><p><strong>Results: </strong>SL-S was feasible in 70% of patients and demonstrated excellent intra- and interobserver reproducibility for both manual and automatic methods. Intraobserver reproducibility for automatic SL-S: ICC 0.97 (CI: 0.94-0.99), BA 0.26 (-1.89 to 2.40) and interobserver reproducibility: ICC 0.96 (CI: 0.92-0.98), and BA 0.53 (-2.41 to 3.47). The reproducibility of manual SL-S was comparable to automatic measurements. Additionally, the reproducibility per chamber was excellent. LVEF was feasible in 80% of patients. Manual LVEF (Simpson's biplane) reproducibility demonstrated good reproducibility: intraobserver ICC: 0.82 (CI: 0.48-0.93), BA -5.00 (-19.70 to 9.70); interobserver ICC 0.78 (CI: 0.55-0.91), BA 7.50 (-5.40 to 20.40). Automatic LVEF (auto-LVEF) demonstrated excellent reproducibility: intraobserver ICC: 0.94 (CI: 0.86-0.98), BA -0.95 (-10.02 to 8.13); and interobserver ICC: 0.94 (CI: 0.87-0.97), BA 1.75 (-6.38 to 10.33).</p><p><strong>Conclusion: </strong>SL-S (global and per chamber) and auto-LVEF were feasible and showed excellent reproducibility. LVEF demonstrated the highest feasibility, while SL-S exhibited the greatest reproducibility. These parameters may represent a useful tool in the evaluation of LV function in ICU patients under IMV.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"62"},"PeriodicalIF":2.8000,"publicationDate":"2025-06-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12173981/pdf/","citationCount":"0","resultStr":"{\"title\":\"Left ventricular systolic longitudinal strain in mechanically ventilated patients in the intensive care unit: assessment of global and chamber reproducibility.\",\"authors\":\"Matías Pécora, Piero Pastorini, Roberto Farolini, Gastón Burghi, F Javier Hurtado\",\"doi\":\"10.1186/s40635-025-00770-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>In the intensive care unit (ICU), left ventricular systolic function is traditionally assessed by measuring the left ventricular ejection fraction (LVEF). Recently, left ventricular global systolic longitudinal strain (SL-S) has emerged as a more sensitive marker of myocardial function in this setting. However, obtaining high-quality echocardiographic images remains a significant challenge, particularly in patients undergoing invasive mechanical ventilation (IMV), and data on the feasibility and reproducibility of these measurements in critically ill patients are limited.</p><p><strong>Objective: </strong>To assess the feasibility and reproducibility (both global and per chamber) of SL-S and LVEF (both manual and automatic) in ICU patients under IMV.</p><p><strong>Materials and methods: </strong>Thirty ICU patients receiving IMV were randomly selected. The feasibility and reproducibility of SL-S (global and per chamber) and LVEF were assessed using both manual and automatic methods. The analysis was performed using the intraclass correlation coefficient (ICC) with its 95% confidence interval (CI), and Bland-Altman analysis (BA), which reported the mean difference and limits of agreement (lower-upper limits of agreement).</p><p><strong>Results: </strong>SL-S was feasible in 70% of patients and demonstrated excellent intra- and interobserver reproducibility for both manual and automatic methods. Intraobserver reproducibility for automatic SL-S: ICC 0.97 (CI: 0.94-0.99), BA 0.26 (-1.89 to 2.40) and interobserver reproducibility: ICC 0.96 (CI: 0.92-0.98), and BA 0.53 (-2.41 to 3.47). The reproducibility of manual SL-S was comparable to automatic measurements. Additionally, the reproducibility per chamber was excellent. LVEF was feasible in 80% of patients. Manual LVEF (Simpson's biplane) reproducibility demonstrated good reproducibility: intraobserver ICC: 0.82 (CI: 0.48-0.93), BA -5.00 (-19.70 to 9.70); interobserver ICC 0.78 (CI: 0.55-0.91), BA 7.50 (-5.40 to 20.40). Automatic LVEF (auto-LVEF) demonstrated excellent reproducibility: intraobserver ICC: 0.94 (CI: 0.86-0.98), BA -0.95 (-10.02 to 8.13); and interobserver ICC: 0.94 (CI: 0.87-0.97), BA 1.75 (-6.38 to 10.33).</p><p><strong>Conclusion: </strong>SL-S (global and per chamber) and auto-LVEF were feasible and showed excellent reproducibility. LVEF demonstrated the highest feasibility, while SL-S exhibited the greatest reproducibility. These parameters may represent a useful tool in the evaluation of LV function in ICU patients under IMV.</p>\",\"PeriodicalId\":13750,\"journal\":{\"name\":\"Intensive Care Medicine Experimental\",\"volume\":\"13 1\",\"pages\":\"62\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-06-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12173981/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Intensive Care Medicine Experimental\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40635-025-00770-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00770-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
摘要
在重症监护病房(ICU),传统上通过测量左心室射血分数(LVEF)来评估左心室收缩功能。最近,在这种情况下,左心室整体收缩纵向应变(SL-S)已成为一种更敏感的心肌功能标志物。然而,获得高质量的超声心动图图像仍然是一个重大挑战,特别是在接受有创机械通气(IMV)的患者中,而且这些测量在危重患者中的可行性和可重复性数据有限。目的:评价SL-S和LVEF(手动和自动)在IMV下ICU患者中的可行性和重复性(整体和单室)。材料与方法:随机选择30例ICU患者接受IMV治疗。采用手动和自动两种方法对SL-S(整体和每个腔室)和LVEF的可行性和再现性进行了评估。分析采用类内相关系数(ICC)及其95%置信区间(CI)和Bland-Altman分析(BA)进行,后者报告了平均差异和一致性限(一致性的上下限)。结果:SL-S在70%的患者中是可行的,并且在手动和自动方法中表现出良好的观察者内部和观察者之间的重复性。自动SL-S的观察者内再现性:ICC 0.97 (CI: 0.94-0.99), BA 0.26(-1.89 - 2.40),观察者间再现性:ICC 0.96 (CI: 0.92-0.98), BA 0.53(-2.41 - 3.47)。手动SL-S的重现性与自动测量相当。此外,每个腔室的重现性很好。80%的患者LVEF是可行的。手动LVEF (Simpson’s biplane)重现性良好:观察者内ICC: 0.82 (CI: 0.48 ~ 0.93), BA -5.00 (-19.70 ~ 9.70);观察者间ICC 0.78 (CI: 0.55-0.91), BA 7.50(-5.40至20.40)。自动LVEF (auto-LVEF)表现出良好的再现性:观察者内ICC: 0.94 (CI: 0.86-0.98), BA -0.95 (-10.02 ~ 8.13);观察者间ICC: 0.94 (CI: 0.87-0.97), BA: 1.75(-6.38 - 10.33)。结论:SL-S(全局和单室)和auto-LVEF是可行的,重现性好。LVEF的可行性最高,SL-S的重现性最高。这些参数可能是评价IMV下ICU患者左室功能的有用工具。
Left ventricular systolic longitudinal strain in mechanically ventilated patients in the intensive care unit: assessment of global and chamber reproducibility.
Introduction: In the intensive care unit (ICU), left ventricular systolic function is traditionally assessed by measuring the left ventricular ejection fraction (LVEF). Recently, left ventricular global systolic longitudinal strain (SL-S) has emerged as a more sensitive marker of myocardial function in this setting. However, obtaining high-quality echocardiographic images remains a significant challenge, particularly in patients undergoing invasive mechanical ventilation (IMV), and data on the feasibility and reproducibility of these measurements in critically ill patients are limited.
Objective: To assess the feasibility and reproducibility (both global and per chamber) of SL-S and LVEF (both manual and automatic) in ICU patients under IMV.
Materials and methods: Thirty ICU patients receiving IMV were randomly selected. The feasibility and reproducibility of SL-S (global and per chamber) and LVEF were assessed using both manual and automatic methods. The analysis was performed using the intraclass correlation coefficient (ICC) with its 95% confidence interval (CI), and Bland-Altman analysis (BA), which reported the mean difference and limits of agreement (lower-upper limits of agreement).
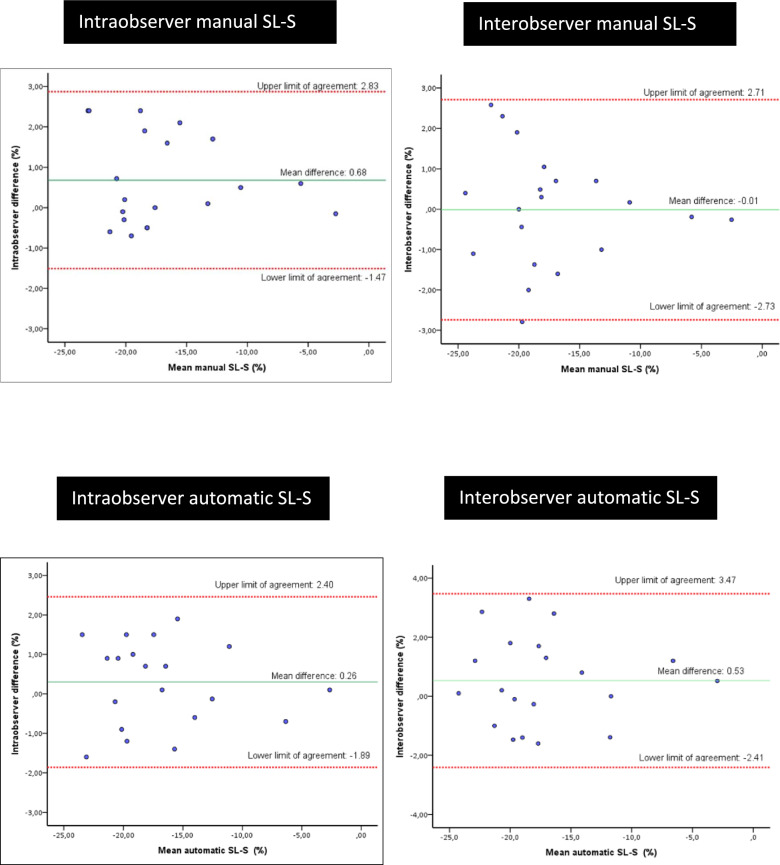
Results: SL-S was feasible in 70% of patients and demonstrated excellent intra- and interobserver reproducibility for both manual and automatic methods. Intraobserver reproducibility for automatic SL-S: ICC 0.97 (CI: 0.94-0.99), BA 0.26 (-1.89 to 2.40) and interobserver reproducibility: ICC 0.96 (CI: 0.92-0.98), and BA 0.53 (-2.41 to 3.47). The reproducibility of manual SL-S was comparable to automatic measurements. Additionally, the reproducibility per chamber was excellent. LVEF was feasible in 80% of patients. Manual LVEF (Simpson's biplane) reproducibility demonstrated good reproducibility: intraobserver ICC: 0.82 (CI: 0.48-0.93), BA -5.00 (-19.70 to 9.70); interobserver ICC 0.78 (CI: 0.55-0.91), BA 7.50 (-5.40 to 20.40). Automatic LVEF (auto-LVEF) demonstrated excellent reproducibility: intraobserver ICC: 0.94 (CI: 0.86-0.98), BA -0.95 (-10.02 to 8.13); and interobserver ICC: 0.94 (CI: 0.87-0.97), BA 1.75 (-6.38 to 10.33).
Conclusion: SL-S (global and per chamber) and auto-LVEF were feasible and showed excellent reproducibility. LVEF demonstrated the highest feasibility, while SL-S exhibited the greatest reproducibility. These parameters may represent a useful tool in the evaluation of LV function in ICU patients under IMV.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


