{"title":"用个体化剂量法评估中晚期肝细胞癌Y90 TARE术后肝切除结果:重点关注手术和胆道并发症","authors":"Mohamad Azhar Meerun, Carole Allimant, Valentina Schembri, Margaux Hermida, Christine Latry-Kuhn, Denis Mariano-Goulart, Fabrizio Panaro, Boris Guiu","doi":"10.21037/hbsn-24-151","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While preliminary reports on resection following downstaging using transarterial radioembolization (TARE) for intermediate or advanced hepatocellular carcinomas (HCCs) reported promising oncological outcomes, there's a notable gap in the literature concerning post operative morbidity. Contrary to post hepatectomy liver failure (PHLF), damages to the bile ducts and their potential consequences have been poorly evaluated. Thus, our aim was to explore postoperative complications in HCC patients undergoing liver resection after Y90 TARE, focusing particularly on biliary complications.</p><p><strong>Methods: </strong>Conducted from June 2015 to December 2022, this retrospective study involved 30 HCC patients undergoing liver resection post-TARE. Comprehensive data on surgical procedures, complications, and follow-up were collected. Logistic regression analyses were conducted, starting with univariate analysis followed by multivariate analysis, focusing on variables with a significance level below P<0.2.</p><p><strong>Results: </strong>The objective response rate (ORR) in the TARE-treated area was 97% at 3 months. Survival outcomes showed a median overall survival (OS) of 5.1 years and progression-free survival (PFS) of 3.5 years post-liver resection. The study found a 40% (12 out of 30 patients) rate of severe postoperative complications and a 7% (2 out of 30 patients) 90-day mortality rate. After liver resection, grade B bile leaks occurred in 20% (6 out of 30) of patients, with a third experiencing recurrence. Biliary-specific mortality was 9%. After multivariate analysis, only the interval between TARE and surgery emerged a significant risk factor for biliary complications, showing increased odds of bile leaks if surgery occurred 3-6 months post-TARE compared to after 6 months.</p><p><strong>Conclusions: </strong>This study highlights the importance of timing between TARE and surgery, suggesting a waiting period of at least 6 months. Such timing not only enhances the radiation effects of TARE but also optimizes both future liver remnant growth and patient selection.</p>","PeriodicalId":12878,"journal":{"name":"Hepatobiliary surgery and nutrition","volume":"14 3","pages":"398-410"},"PeriodicalIF":7.8000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12170090/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluating liver resection outcomes post Y90 TARE with personalized dosimetry in intermediate or advanced hepatocellular carcinoma: a focus on surgical and biliary complications.\",\"authors\":\"Mohamad Azhar Meerun, Carole Allimant, Valentina Schembri, Margaux Hermida, Christine Latry-Kuhn, Denis Mariano-Goulart, Fabrizio Panaro, Boris Guiu\",\"doi\":\"10.21037/hbsn-24-151\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>While preliminary reports on resection following downstaging using transarterial radioembolization (TARE) for intermediate or advanced hepatocellular carcinomas (HCCs) reported promising oncological outcomes, there's a notable gap in the literature concerning post operative morbidity. Contrary to post hepatectomy liver failure (PHLF), damages to the bile ducts and their potential consequences have been poorly evaluated. Thus, our aim was to explore postoperative complications in HCC patients undergoing liver resection after Y90 TARE, focusing particularly on biliary complications.</p><p><strong>Methods: </strong>Conducted from June 2015 to December 2022, this retrospective study involved 30 HCC patients undergoing liver resection post-TARE. Comprehensive data on surgical procedures, complications, and follow-up were collected. Logistic regression analyses were conducted, starting with univariate analysis followed by multivariate analysis, focusing on variables with a significance level below P<0.2.</p><p><strong>Results: </strong>The objective response rate (ORR) in the TARE-treated area was 97% at 3 months. Survival outcomes showed a median overall survival (OS) of 5.1 years and progression-free survival (PFS) of 3.5 years post-liver resection. The study found a 40% (12 out of 30 patients) rate of severe postoperative complications and a 7% (2 out of 30 patients) 90-day mortality rate. After liver resection, grade B bile leaks occurred in 20% (6 out of 30) of patients, with a third experiencing recurrence. Biliary-specific mortality was 9%. After multivariate analysis, only the interval between TARE and surgery emerged a significant risk factor for biliary complications, showing increased odds of bile leaks if surgery occurred 3-6 months post-TARE compared to after 6 months.</p><p><strong>Conclusions: </strong>This study highlights the importance of timing between TARE and surgery, suggesting a waiting period of at least 6 months. Such timing not only enhances the radiation effects of TARE but also optimizes both future liver remnant growth and patient selection.</p>\",\"PeriodicalId\":12878,\"journal\":{\"name\":\"Hepatobiliary surgery and nutrition\",\"volume\":\"14 3\",\"pages\":\"398-410\"},\"PeriodicalIF\":7.8000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12170090/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hepatobiliary surgery and nutrition\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/hbsn-24-151\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/11/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatobiliary surgery and nutrition","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/hbsn-24-151","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Evaluating liver resection outcomes post Y90 TARE with personalized dosimetry in intermediate or advanced hepatocellular carcinoma: a focus on surgical and biliary complications.
Background: While preliminary reports on resection following downstaging using transarterial radioembolization (TARE) for intermediate or advanced hepatocellular carcinomas (HCCs) reported promising oncological outcomes, there's a notable gap in the literature concerning post operative morbidity. Contrary to post hepatectomy liver failure (PHLF), damages to the bile ducts and their potential consequences have been poorly evaluated. Thus, our aim was to explore postoperative complications in HCC patients undergoing liver resection after Y90 TARE, focusing particularly on biliary complications.
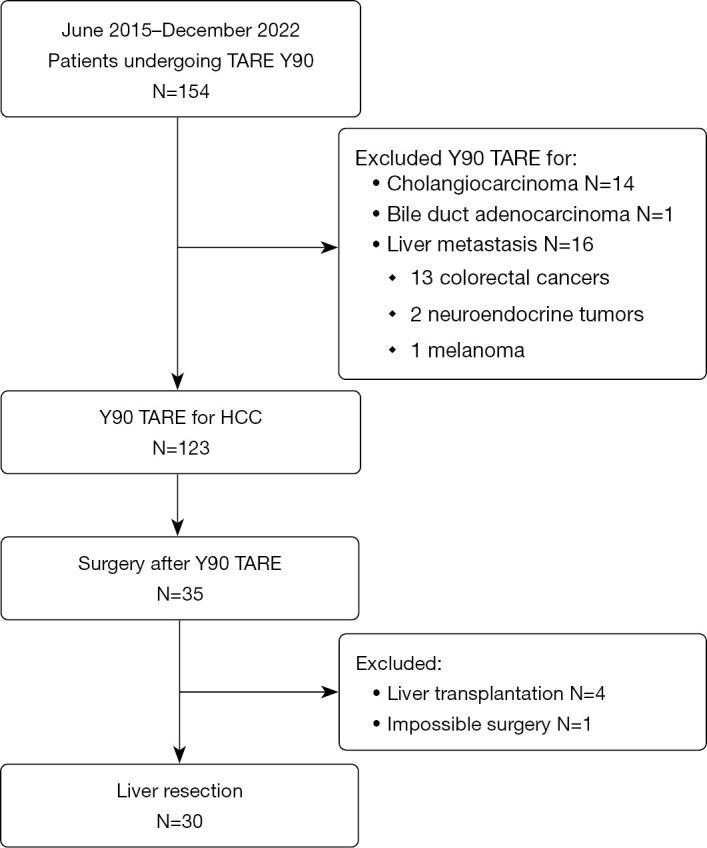
Methods: Conducted from June 2015 to December 2022, this retrospective study involved 30 HCC patients undergoing liver resection post-TARE. Comprehensive data on surgical procedures, complications, and follow-up were collected. Logistic regression analyses were conducted, starting with univariate analysis followed by multivariate analysis, focusing on variables with a significance level below P<0.2.
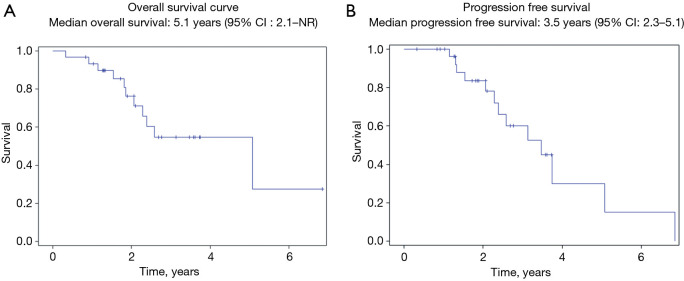
Results: The objective response rate (ORR) in the TARE-treated area was 97% at 3 months. Survival outcomes showed a median overall survival (OS) of 5.1 years and progression-free survival (PFS) of 3.5 years post-liver resection. The study found a 40% (12 out of 30 patients) rate of severe postoperative complications and a 7% (2 out of 30 patients) 90-day mortality rate. After liver resection, grade B bile leaks occurred in 20% (6 out of 30) of patients, with a third experiencing recurrence. Biliary-specific mortality was 9%. After multivariate analysis, only the interval between TARE and surgery emerged a significant risk factor for biliary complications, showing increased odds of bile leaks if surgery occurred 3-6 months post-TARE compared to after 6 months.
Conclusions: This study highlights the importance of timing between TARE and surgery, suggesting a waiting period of at least 6 months. Such timing not only enhances the radiation effects of TARE but also optimizes both future liver remnant growth and patient selection.
期刊介绍:
Hepatobiliary Surgery and Nutrition (HBSN) is a bi-monthly, open-access, peer-reviewed journal (Print ISSN: 2304-3881; Online ISSN: 2304-389X) since December 2012. The journal focuses on hepatopancreatobiliary disease and nutrition, aiming to present new findings and deliver up-to-date, practical information on diagnosis, prevention, and clinical investigations. Areas of interest cover surgical techniques, clinical and basic research, transplantation, therapies, NASH, NAFLD, targeted drugs, gut microbiota, metabolism, cancer immunity, genomics, and nutrition and dietetics. HBSN serves as a valuable resource for professionals seeking insights into diverse aspects of hepatobiliary surgery and nutrition.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


