{"title":"免疫相关性暴发性心肌炎在晚期肾细胞癌治疗中尸检心肌组织病理学显示:1例报告。","authors":"Yuka Hayashi, Yoshihide Kawasaki, Hiromichi Katayama, Rie Sakagami, Takuro Goto, Tomonori Sato, Yohei Satake, Takuma Sato, Naoki Kawamorita, Shinichi Yamashita, Hiroyuki Takahama, Satoko Sato, Akihiro Ito","doi":"10.1159/000546288","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Although immune checkpoint inhibitor-associated myocarditis is relatively rare, it has the highest mortality rate among all immune-related adverse events, at 30-50%.</p><p><strong>Case presentation: </strong>We encountered a case of advanced renal cancer in which immune checkpoint inhibitor-associated myocarditis was confirmed on autopsy. A 78-year-old man was diagnosed with a left renal tumor secondary to hematuria. A tumor biopsy was performed, and the tumor was diagnosed as cT4N0M1 clear cell renal carcinoma, which was classified as poor risk by the International mRCC Database Consortium. Combination therapy with pembrolizumab and axitinib was initiated. One month later, the patient developed anorexia, dizziness, and fatigue, which were judged to be adverse events due to systemic therapy, and the patient was admitted to the hospital urgently. After admission, the patient experienced a sudden drop in blood pressure and loss of consciousness and was referred to a cardiologist for treatment. Blood tests showed elevated brain-type natriuretic peptide levels, but echocardiography showed good cardiac function. However, soon thereafter, the patient developed tachycardia, and echocardiography revealed a significant decline in systolic function, leading to the diagnosis of immune checkpoint inhibitor-associated myocarditis. Despite intensive care in the cardiac high-care unit and steroid administration, the patient died. An autopsy revealed necrotic changes in the myocardium, loss of myocardial cells, and severe lymphocyte infiltration, leading to a diagnosis of inhibitor-associated myocarditis.</p><p><strong>Conclusion: </strong>Delay in the initiation of treatment is considered a risk factor for poor prognosis, and the administration of high-dose steroids within 24 h of onset contributes to a better outcome. Herein, we discuss the pathology, diagnosis, and treatment of immune checkpoint inhibitor-associated myocarditis.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"738-743"},"PeriodicalIF":0.7000,"publicationDate":"2025-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12165635/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immune-Related Fulminant Myocarditis Revealed Using Myocardial Histopathology at Autopsy in the Treatment of Advanced Renal Cell Carcinoma: A Case Report.\",\"authors\":\"Yuka Hayashi, Yoshihide Kawasaki, Hiromichi Katayama, Rie Sakagami, Takuro Goto, Tomonori Sato, Yohei Satake, Takuma Sato, Naoki Kawamorita, Shinichi Yamashita, Hiroyuki Takahama, Satoko Sato, Akihiro Ito\",\"doi\":\"10.1159/000546288\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Although immune checkpoint inhibitor-associated myocarditis is relatively rare, it has the highest mortality rate among all immune-related adverse events, at 30-50%.</p><p><strong>Case presentation: </strong>We encountered a case of advanced renal cancer in which immune checkpoint inhibitor-associated myocarditis was confirmed on autopsy. A 78-year-old man was diagnosed with a left renal tumor secondary to hematuria. A tumor biopsy was performed, and the tumor was diagnosed as cT4N0M1 clear cell renal carcinoma, which was classified as poor risk by the International mRCC Database Consortium. Combination therapy with pembrolizumab and axitinib was initiated. One month later, the patient developed anorexia, dizziness, and fatigue, which were judged to be adverse events due to systemic therapy, and the patient was admitted to the hospital urgently. After admission, the patient experienced a sudden drop in blood pressure and loss of consciousness and was referred to a cardiologist for treatment. Blood tests showed elevated brain-type natriuretic peptide levels, but echocardiography showed good cardiac function. However, soon thereafter, the patient developed tachycardia, and echocardiography revealed a significant decline in systolic function, leading to the diagnosis of immune checkpoint inhibitor-associated myocarditis. Despite intensive care in the cardiac high-care unit and steroid administration, the patient died. An autopsy revealed necrotic changes in the myocardium, loss of myocardial cells, and severe lymphocyte infiltration, leading to a diagnosis of inhibitor-associated myocarditis.</p><p><strong>Conclusion: </strong>Delay in the initiation of treatment is considered a risk factor for poor prognosis, and the administration of high-dose steroids within 24 h of onset contributes to a better outcome. Herein, we discuss the pathology, diagnosis, and treatment of immune checkpoint inhibitor-associated myocarditis.</p>\",\"PeriodicalId\":9625,\"journal\":{\"name\":\"Case Reports in Oncology\",\"volume\":\"18 1\",\"pages\":\"738-743\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12165635/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000546288\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000546288","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Immune-Related Fulminant Myocarditis Revealed Using Myocardial Histopathology at Autopsy in the Treatment of Advanced Renal Cell Carcinoma: A Case Report.
Introduction: Although immune checkpoint inhibitor-associated myocarditis is relatively rare, it has the highest mortality rate among all immune-related adverse events, at 30-50%.
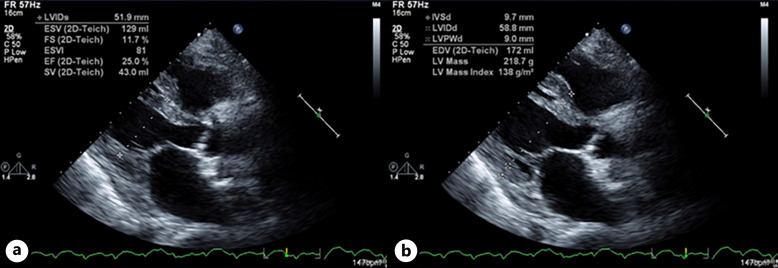
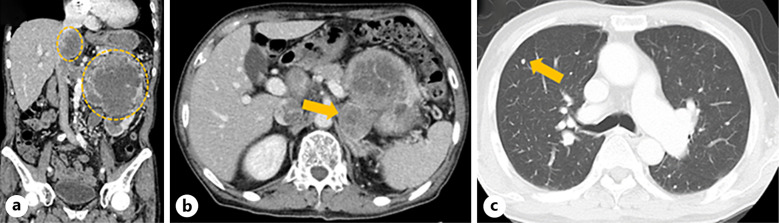
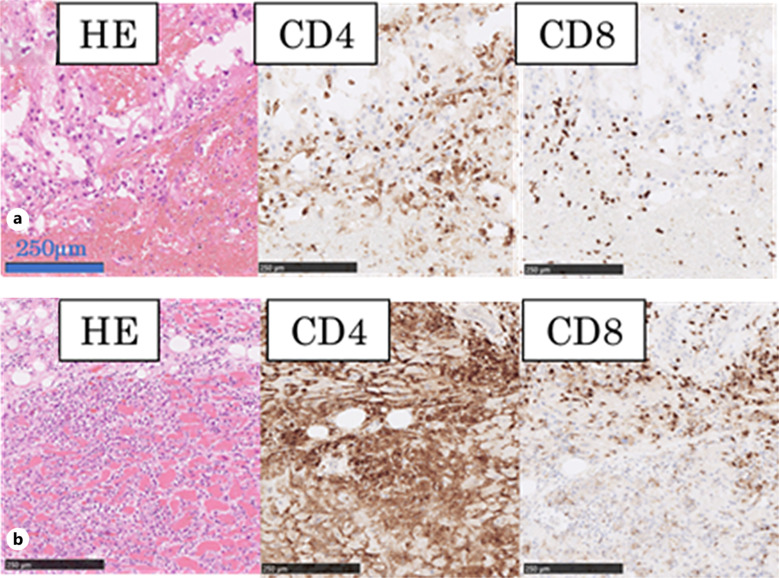
Case presentation: We encountered a case of advanced renal cancer in which immune checkpoint inhibitor-associated myocarditis was confirmed on autopsy. A 78-year-old man was diagnosed with a left renal tumor secondary to hematuria. A tumor biopsy was performed, and the tumor was diagnosed as cT4N0M1 clear cell renal carcinoma, which was classified as poor risk by the International mRCC Database Consortium. Combination therapy with pembrolizumab and axitinib was initiated. One month later, the patient developed anorexia, dizziness, and fatigue, which were judged to be adverse events due to systemic therapy, and the patient was admitted to the hospital urgently. After admission, the patient experienced a sudden drop in blood pressure and loss of consciousness and was referred to a cardiologist for treatment. Blood tests showed elevated brain-type natriuretic peptide levels, but echocardiography showed good cardiac function. However, soon thereafter, the patient developed tachycardia, and echocardiography revealed a significant decline in systolic function, leading to the diagnosis of immune checkpoint inhibitor-associated myocarditis. Despite intensive care in the cardiac high-care unit and steroid administration, the patient died. An autopsy revealed necrotic changes in the myocardium, loss of myocardial cells, and severe lymphocyte infiltration, leading to a diagnosis of inhibitor-associated myocarditis.
Conclusion: Delay in the initiation of treatment is considered a risk factor for poor prognosis, and the administration of high-dose steroids within 24 h of onset contributes to a better outcome. Herein, we discuss the pathology, diagnosis, and treatment of immune checkpoint inhibitor-associated myocarditis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


