Sandy Burmeister, Katarzyna Jóźwiak, Christiane Richter-Ehrenstein, André Buchali, Christine Holmberg, Anne von Rüsten, Constanze Schneider, Michael Hauptmann
{"title":"2007-2020年期间,德国联邦州柏林和勃兰登堡州导管原位癌的治疗和预后","authors":"Sandy Burmeister, Katarzyna Jóźwiak, Christiane Richter-Ehrenstein, André Buchali, Christine Holmberg, Anne von Rüsten, Constanze Schneider, Michael Hauptmann","doi":"10.1055/a-2505-1682","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ductal carcinoma in situ (DCIS) of the female breast is treated with surgery possibly followed by radiotherapy (RT) and/or adjuvant hormonal therapy despite their known long-term side effects. Since not every DCIS will progress into an invasive breast cancer (IBC), disease progression and de-escalation of treatment is an important topic of current research.</p><p><strong>Methods: </strong>During 2007-2020, 3905 individuals with a DCIS diagnosis were reported to the cancer registry of Brandenburg and Berlin. We selected 3424 women who were cancer-free prior to DCIS diagnosis and without synchronous diagnoses of DCIS or ipsilateral IBC (iIBC). The objective was to describe changes over time in DCIS treatment and risk of developing iIBC by treatment.</p><p><strong>Results: </strong>We observed decreasing proportions of mastectomy, breast-conserving surgery (BCS) with RT, and standard versus hypofractionated RT over time. During a median follow-up of 3.8 years, 105 women developed iIBC. Compared with BCS + RT with standard fractionation (54.9%, 1878/3424, 53 iIBC events), hazard ratios (HR) for ilBC were 0.72 (95% confidence interval [CI] 0.26, 1.99; 4 events) for BCS + hypofractionated RT, 0.70 (95% CI 0.33, 1.41; 11 events) for BCS alone, and 0.83 (95% CI 0.50, 1.37; 26 events) for mastectomy. Analyses were adjusted for DCIS size, grade, residual tumor status and ECOG score.</p><p><strong>Conclusion: </strong>We observed a de-escalation of treatment over time, with fewer mastectomies, less RT, and more hypofractionation of RT. No substantial differences in risk of iIBC were observed between these treatments. There is a need to evaluate DCIS treatment de-escalation in larger cohorts with longer follow-up.</p>","PeriodicalId":12481,"journal":{"name":"Geburtshilfe Und Frauenheilkunde","volume":"85 6","pages":"620-630"},"PeriodicalIF":1.9000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12158539/pdf/","citationCount":"0","resultStr":"{\"title\":\"Treatment and Outcome of Ductal Carcinoma in Situ for the German Federal States Berlin and Brandenburg in the Period 2007-2020.\",\"authors\":\"Sandy Burmeister, Katarzyna Jóźwiak, Christiane Richter-Ehrenstein, André Buchali, Christine Holmberg, Anne von Rüsten, Constanze Schneider, Michael Hauptmann\",\"doi\":\"10.1055/a-2505-1682\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ductal carcinoma in situ (DCIS) of the female breast is treated with surgery possibly followed by radiotherapy (RT) and/or adjuvant hormonal therapy despite their known long-term side effects. Since not every DCIS will progress into an invasive breast cancer (IBC), disease progression and de-escalation of treatment is an important topic of current research.</p><p><strong>Methods: </strong>During 2007-2020, 3905 individuals with a DCIS diagnosis were reported to the cancer registry of Brandenburg and Berlin. We selected 3424 women who were cancer-free prior to DCIS diagnosis and without synchronous diagnoses of DCIS or ipsilateral IBC (iIBC). The objective was to describe changes over time in DCIS treatment and risk of developing iIBC by treatment.</p><p><strong>Results: </strong>We observed decreasing proportions of mastectomy, breast-conserving surgery (BCS) with RT, and standard versus hypofractionated RT over time. During a median follow-up of 3.8 years, 105 women developed iIBC. Compared with BCS + RT with standard fractionation (54.9%, 1878/3424, 53 iIBC events), hazard ratios (HR) for ilBC were 0.72 (95% confidence interval [CI] 0.26, 1.99; 4 events) for BCS + hypofractionated RT, 0.70 (95% CI 0.33, 1.41; 11 events) for BCS alone, and 0.83 (95% CI 0.50, 1.37; 26 events) for mastectomy. Analyses were adjusted for DCIS size, grade, residual tumor status and ECOG score.</p><p><strong>Conclusion: </strong>We observed a de-escalation of treatment over time, with fewer mastectomies, less RT, and more hypofractionation of RT. No substantial differences in risk of iIBC were observed between these treatments. There is a need to evaluate DCIS treatment de-escalation in larger cohorts with longer follow-up.</p>\",\"PeriodicalId\":12481,\"journal\":{\"name\":\"Geburtshilfe Und Frauenheilkunde\",\"volume\":\"85 6\",\"pages\":\"620-630\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2025-01-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12158539/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Geburtshilfe Und Frauenheilkunde\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2505-1682\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geburtshilfe Und Frauenheilkunde","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2505-1682","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:女性乳腺导管原位癌(DCIS)的治疗通常采用手术治疗,放疗(RT)和/或辅助激素治疗,尽管其已知的长期副作用。由于并非每个DCIS都会发展为浸润性乳腺癌(IBC),因此疾病进展和治疗降级是当前研究的重要课题。方法:2007-2020年期间,在勃兰登堡和柏林的癌症登记处报告了3905例DCIS诊断。我们选择了3424名在DCIS诊断前无癌且未同时诊断DCIS或同侧IBC (iIBC)的女性。目的是描述DCIS治疗随时间的变化和治疗后发生iIBC的风险。结果:我们观察到随着时间的推移,乳房切除术、保乳手术(BCS)和标准RT与低分割RT的比例在下降。在中位3.8年的随访期间,105名女性发展为iIBC。与标准分馏的BCS + RT (54.9%, 1878/3424, 53 iIBC事件)相比,ilBC的风险比(HR)为0.72(95%可信区间[CI] 0.26, 1.99;4个事件),BCS +低分割RT为0.70 (95% CI 0.33, 1.41;11个事件)和0.83 (95% CI 0.50, 1.37;26例)。对DCIS大小、分级、残留肿瘤状态和ECOG评分进行校正分析。结论:随着时间的推移,我们观察到治疗的降级,更少的乳房切除术,更少的放疗和更多的低分割放疗。这些治疗之间没有观察到iIBC风险的实质性差异。有必要在更大的随访时间更长的队列中评估DCIS治疗的降级。
Treatment and Outcome of Ductal Carcinoma in Situ for the German Federal States Berlin and Brandenburg in the Period 2007-2020.
Background: Ductal carcinoma in situ (DCIS) of the female breast is treated with surgery possibly followed by radiotherapy (RT) and/or adjuvant hormonal therapy despite their known long-term side effects. Since not every DCIS will progress into an invasive breast cancer (IBC), disease progression and de-escalation of treatment is an important topic of current research.
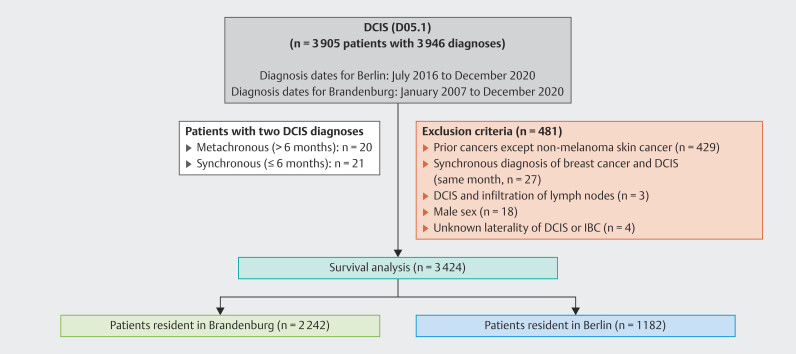
Methods: During 2007-2020, 3905 individuals with a DCIS diagnosis were reported to the cancer registry of Brandenburg and Berlin. We selected 3424 women who were cancer-free prior to DCIS diagnosis and without synchronous diagnoses of DCIS or ipsilateral IBC (iIBC). The objective was to describe changes over time in DCIS treatment and risk of developing iIBC by treatment.
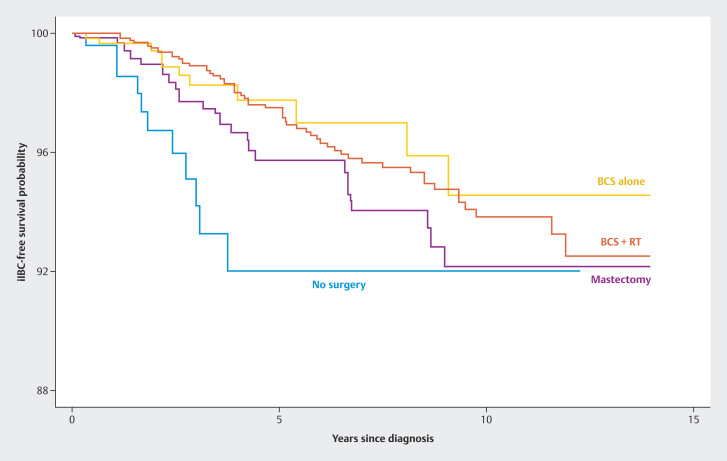
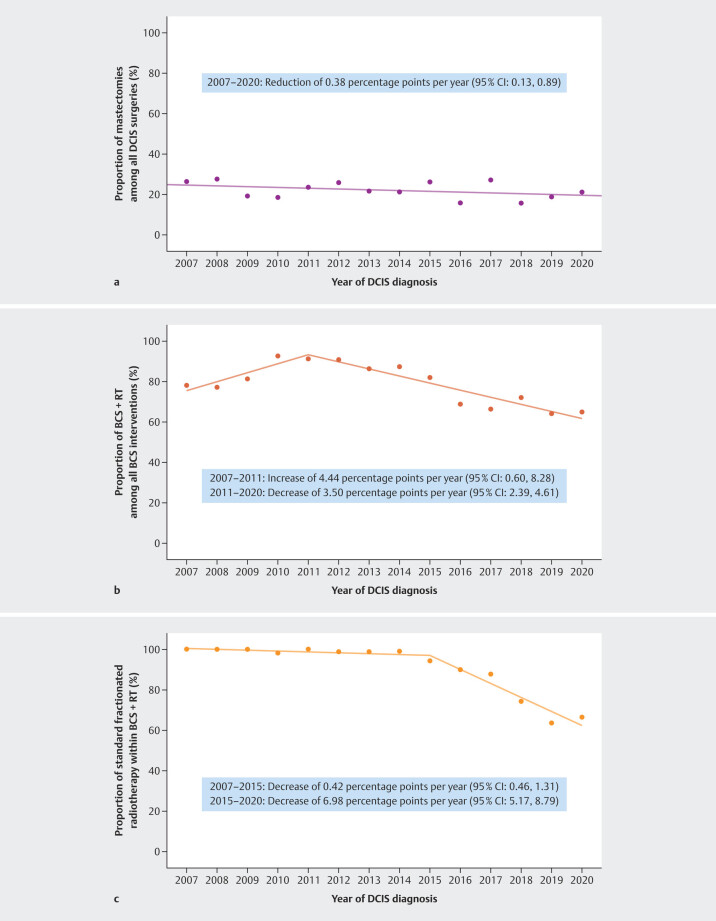
Results: We observed decreasing proportions of mastectomy, breast-conserving surgery (BCS) with RT, and standard versus hypofractionated RT over time. During a median follow-up of 3.8 years, 105 women developed iIBC. Compared with BCS + RT with standard fractionation (54.9%, 1878/3424, 53 iIBC events), hazard ratios (HR) for ilBC were 0.72 (95% confidence interval [CI] 0.26, 1.99; 4 events) for BCS + hypofractionated RT, 0.70 (95% CI 0.33, 1.41; 11 events) for BCS alone, and 0.83 (95% CI 0.50, 1.37; 26 events) for mastectomy. Analyses were adjusted for DCIS size, grade, residual tumor status and ECOG score.
Conclusion: We observed a de-escalation of treatment over time, with fewer mastectomies, less RT, and more hypofractionation of RT. No substantial differences in risk of iIBC were observed between these treatments. There is a need to evaluate DCIS treatment de-escalation in larger cohorts with longer follow-up.
期刊介绍:
Geburtshilfe und Frauenheilkunde (GebFra) addresses the whole field of obstetrics and gynecology and is concerned with research as much as with clinical practice. In its scientific section, it publishes original articles, reviews and case reports in all fields of the discipline, namely
gynecological oncology, including oncology of the breast
obstetrics and perinatal medicine,
reproductive medicine,
and urogynecology.
GebFra invites the submission of original articles and review articles.
In addition, the journal publishes guidelines, statements and recommendations in cooperation with the DGGG, SGGG, OEGGG and the Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF, Association of Scientific Medical Societies, www.awmf.org). Apart from the scientific section, Geburtshilfe und Frauenheilkunde has a news and views section that also includes discussions, book reviews and professional information.
Letters to the editors are welcome. If a letter discusses an article that has been published in our journal, the corresponding author of the article will be informed and invited to comment on the letter. The comment will be published along with the letter.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


