{"title":"计算机断层扫描引导下的经皮活检评估神经内分泌肿瘤转移到肝脏的肿瘤异质性。","authors":"Lei-Lei Ying, Ke-Ning Li, Wen-Tao Li, Xin-Hong He, Chao Chen","doi":"10.4329/wjr.v17.i5.104808","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Gastroenteropancreatic neuroendocrine tumors (GEP-NETs) frequently metastasize to the liver, with heterogeneity in tumor grade impacting patient prognosis and treatment. The Ki-67 index, a key prognostic marker, often varies between primary and metastatic sites; however, routine liver biopsy remains controversial. Although percutaneous computed tomography-guided core needle biopsy (PCT-CNB) is safe and effective for focal lesions, its role in detecting intertumor grading discrepancies and survival implications in GEP-NETs is underexplored. Conflicting survival associations with grade shifts have been reported in previous studies. We hypothesized that PCT-CNB could identify clinically significant grading heterogeneity in liver metastases, correlating with survival outcomes, thereby refining risk stratification and therapeutic strategies.</p><p><strong>Aim: </strong>To investigate intertumor grading heterogeneity in GEP-NET liver metastases <i>via</i> PCT-CNB.</p><p><strong>Methods: </strong>We retrospectively investigated 92 patients with liver metastases from GEP-NETs <i>via</i> PCT-CNB, 76 patient samples from the liver and primary sites, and 16 from the liver and secondary liver sites. Ki-67 immunohistochemistry was performed for tissue sampling, and grading classifications were determined. Intertumor grading classification heterogeneity and associated changes in patient survival outcomes were also evaluated.</p><p><strong>Results: </strong>No procedure-related mortality was recorded during or after biopsy. In 37/92 patients (40.2%), the grading classifications changed: The grading increased from G1 to G2 in 13 patients, from G1 to G3 in 2, and from G2 to G3 in 14; the grading decreased from G2 to G1 in 5 patients, from G3 to G1 in 1, and from G3 to G2 in 2. Patients with G1 or G2 disease had better progression-free survival and overall survival (OS) outcomes than those with G3 disease did (<i>P</i> = 0.001 and <i>P</i> < 0.001, respectively). The 5-year and 10-year OS rates for stable G2 patients were 67.5% and 26.0%, respectively, decreasing to 46.4% and 23.2%, respectively, among G2 patients whose grade increased (<i>P</i> = 0.016).</p><p><strong>Conclusion: </strong>The PCT-CNB of liver metastases from GEP-NETs differed in grade between the liver tumor and primary site/secondary liver metastases. Additionally, when grading increased from G2, the OS rate significantly decreased.</p>","PeriodicalId":23819,"journal":{"name":"World journal of radiology","volume":"17 5","pages":"104808"},"PeriodicalIF":1.5000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149974/pdf/","citationCount":"0","resultStr":"{\"title\":\"Computed tomography-guided percutaneous biopsy for assessing tumor heterogeneity in neuroendocrine tumor metastases to the liver.\",\"authors\":\"Lei-Lei Ying, Ke-Ning Li, Wen-Tao Li, Xin-Hong He, Chao Chen\",\"doi\":\"10.4329/wjr.v17.i5.104808\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Gastroenteropancreatic neuroendocrine tumors (GEP-NETs) frequently metastasize to the liver, with heterogeneity in tumor grade impacting patient prognosis and treatment. The Ki-67 index, a key prognostic marker, often varies between primary and metastatic sites; however, routine liver biopsy remains controversial. Although percutaneous computed tomography-guided core needle biopsy (PCT-CNB) is safe and effective for focal lesions, its role in detecting intertumor grading discrepancies and survival implications in GEP-NETs is underexplored. Conflicting survival associations with grade shifts have been reported in previous studies. We hypothesized that PCT-CNB could identify clinically significant grading heterogeneity in liver metastases, correlating with survival outcomes, thereby refining risk stratification and therapeutic strategies.</p><p><strong>Aim: </strong>To investigate intertumor grading heterogeneity in GEP-NET liver metastases <i>via</i> PCT-CNB.</p><p><strong>Methods: </strong>We retrospectively investigated 92 patients with liver metastases from GEP-NETs <i>via</i> PCT-CNB, 76 patient samples from the liver and primary sites, and 16 from the liver and secondary liver sites. Ki-67 immunohistochemistry was performed for tissue sampling, and grading classifications were determined. Intertumor grading classification heterogeneity and associated changes in patient survival outcomes were also evaluated.</p><p><strong>Results: </strong>No procedure-related mortality was recorded during or after biopsy. In 37/92 patients (40.2%), the grading classifications changed: The grading increased from G1 to G2 in 13 patients, from G1 to G3 in 2, and from G2 to G3 in 14; the grading decreased from G2 to G1 in 5 patients, from G3 to G1 in 1, and from G3 to G2 in 2. Patients with G1 or G2 disease had better progression-free survival and overall survival (OS) outcomes than those with G3 disease did (<i>P</i> = 0.001 and <i>P</i> < 0.001, respectively). The 5-year and 10-year OS rates for stable G2 patients were 67.5% and 26.0%, respectively, decreasing to 46.4% and 23.2%, respectively, among G2 patients whose grade increased (<i>P</i> = 0.016).</p><p><strong>Conclusion: </strong>The PCT-CNB of liver metastases from GEP-NETs differed in grade between the liver tumor and primary site/secondary liver metastases. Additionally, when grading increased from G2, the OS rate significantly decreased.</p>\",\"PeriodicalId\":23819,\"journal\":{\"name\":\"World journal of radiology\",\"volume\":\"17 5\",\"pages\":\"104808\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149974/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World journal of radiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4329/wjr.v17.i5.104808\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World journal of radiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4329/wjr.v17.i5.104808","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Computed tomography-guided percutaneous biopsy for assessing tumor heterogeneity in neuroendocrine tumor metastases to the liver.
Background: Gastroenteropancreatic neuroendocrine tumors (GEP-NETs) frequently metastasize to the liver, with heterogeneity in tumor grade impacting patient prognosis and treatment. The Ki-67 index, a key prognostic marker, often varies between primary and metastatic sites; however, routine liver biopsy remains controversial. Although percutaneous computed tomography-guided core needle biopsy (PCT-CNB) is safe and effective for focal lesions, its role in detecting intertumor grading discrepancies and survival implications in GEP-NETs is underexplored. Conflicting survival associations with grade shifts have been reported in previous studies. We hypothesized that PCT-CNB could identify clinically significant grading heterogeneity in liver metastases, correlating with survival outcomes, thereby refining risk stratification and therapeutic strategies.
Aim: To investigate intertumor grading heterogeneity in GEP-NET liver metastases via PCT-CNB.
Methods: We retrospectively investigated 92 patients with liver metastases from GEP-NETs via PCT-CNB, 76 patient samples from the liver and primary sites, and 16 from the liver and secondary liver sites. Ki-67 immunohistochemistry was performed for tissue sampling, and grading classifications were determined. Intertumor grading classification heterogeneity and associated changes in patient survival outcomes were also evaluated.
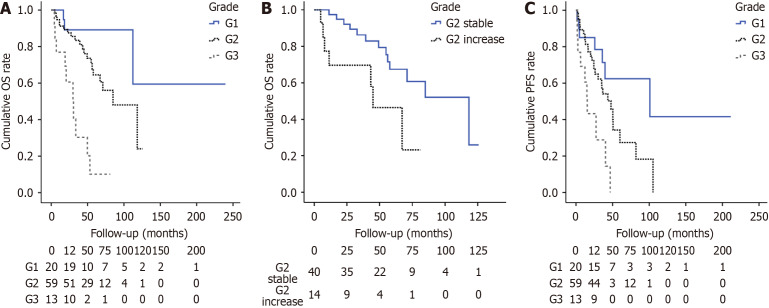
Results: No procedure-related mortality was recorded during or after biopsy. In 37/92 patients (40.2%), the grading classifications changed: The grading increased from G1 to G2 in 13 patients, from G1 to G3 in 2, and from G2 to G3 in 14; the grading decreased from G2 to G1 in 5 patients, from G3 to G1 in 1, and from G3 to G2 in 2. Patients with G1 or G2 disease had better progression-free survival and overall survival (OS) outcomes than those with G3 disease did (P = 0.001 and P < 0.001, respectively). The 5-year and 10-year OS rates for stable G2 patients were 67.5% and 26.0%, respectively, decreasing to 46.4% and 23.2%, respectively, among G2 patients whose grade increased (P = 0.016).
Conclusion: The PCT-CNB of liver metastases from GEP-NETs differed in grade between the liver tumor and primary site/secondary liver metastases. Additionally, when grading increased from G2, the OS rate significantly decreased.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


