Karan J Yagnik, Raj Patel, Sneh Sonaiya, Charmy Parikh, Pranav Patel, Yash Shah, Umar Hayat, Dushyant Singh Dahiya, Dhruvil Radadiya, Hareesha Rishab Bharadwaj, Doantrang Du, Ben Terrany, Dharmesh Kaswala, Bradley Confer, Harshit S Khara
{"title":"医院教学状况对急性胆管炎预后的影响:美国住院倾向匹配分析","authors":"Karan J Yagnik, Raj Patel, Sneh Sonaiya, Charmy Parikh, Pranav Patel, Yash Shah, Umar Hayat, Dushyant Singh Dahiya, Dhruvil Radadiya, Hareesha Rishab Bharadwaj, Doantrang Du, Ben Terrany, Dharmesh Kaswala, Bradley Confer, Harshit S Khara","doi":"10.14740/gr2038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute cholangitis (AC) is a serious condition caused by partial or complete obstruction of the common bile duct (CBD), leading to biliary tract infection. We aimed to evaluate whether teaching hospitals with trainees and non-teaching hospitals impact the outcome of AC in the United States.</p><p><strong>Methods: </strong>This study utilized the National Inpatient Sample database to analyze adult hospitalizations (> 18 years old) with a primary diagnosis of AC in the USA from 2016 to 2020. A multivariate logistic regression along with Chi-square and <i>t</i>-tests was performed using SAS 9.4 software to analyze inpatient AC-associated mortality, inflation-adjusted total hospitalization costs (THC), and length of stay (LOS) in US teaching and non-teaching hospitals during the study period.</p><p><strong>Results: </strong>This study included a total of 30,300 patients, out of whom 23,535 (about 78%) were managed in teaching hospitals and 6,765 (about 22%) were managed in non-teaching hospitals. Primary outcomes showed a significant increase in mortality for patients managed in teaching hospitals (2.77% vs. 2.08%, P = 0.01) in comparison to non-teaching hospitals, hospital LOS was slightly higher in teaching hospitals (5 days (interquartile range (IQR): 3 - 6) vs. 4 days (IQR: 3 - 8)) and so did hospital cost ($15,259 vs. $14,506) in comparison to non-teaching hospitals. Secondary outcomes showed that patients in teaching hospitals had higher incidence of septic shock (16.06% vs. 12.53%, P < 0.0001), intensive care unit (ICU) admissions (6.61% vs. 5.07%, P = 0.0002), and intubation (5.30% vs. 3.46%, P < 0.0001) in comparison to non-teaching hospitals.</p><p><strong>Conclusion: </strong>Our study found higher mortality rates for AC patients in teaching hospitals compared to non-teaching hospitals. Teaching hospitals also had higher rates of septic shock, ICU admission, and intubation, with no difference in endoscopic retrograde cholangiopancreatography (ERCP) use. These differences could be due to several factors, such as greater resident and fellow autonomy in teaching hospitals and a potentially more proactive approach by physicians in non-teaching hospitals. Additionally, teaching hospitals often manage more complex, higher-acuity cases, which could contribute to worse outcomes.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"18 3","pages":"129-138"},"PeriodicalIF":1.7000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151124/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of Hospital Teaching Status on Outcomes of Acute Cholangitis: A Propensity-Matched Analysis of Hospitalizations in the United States.\",\"authors\":\"Karan J Yagnik, Raj Patel, Sneh Sonaiya, Charmy Parikh, Pranav Patel, Yash Shah, Umar Hayat, Dushyant Singh Dahiya, Dhruvil Radadiya, Hareesha Rishab Bharadwaj, Doantrang Du, Ben Terrany, Dharmesh Kaswala, Bradley Confer, Harshit S Khara\",\"doi\":\"10.14740/gr2038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute cholangitis (AC) is a serious condition caused by partial or complete obstruction of the common bile duct (CBD), leading to biliary tract infection. We aimed to evaluate whether teaching hospitals with trainees and non-teaching hospitals impact the outcome of AC in the United States.</p><p><strong>Methods: </strong>This study utilized the National Inpatient Sample database to analyze adult hospitalizations (> 18 years old) with a primary diagnosis of AC in the USA from 2016 to 2020. A multivariate logistic regression along with Chi-square and <i>t</i>-tests was performed using SAS 9.4 software to analyze inpatient AC-associated mortality, inflation-adjusted total hospitalization costs (THC), and length of stay (LOS) in US teaching and non-teaching hospitals during the study period.</p><p><strong>Results: </strong>This study included a total of 30,300 patients, out of whom 23,535 (about 78%) were managed in teaching hospitals and 6,765 (about 22%) were managed in non-teaching hospitals. Primary outcomes showed a significant increase in mortality for patients managed in teaching hospitals (2.77% vs. 2.08%, P = 0.01) in comparison to non-teaching hospitals, hospital LOS was slightly higher in teaching hospitals (5 days (interquartile range (IQR): 3 - 6) vs. 4 days (IQR: 3 - 8)) and so did hospital cost ($15,259 vs. $14,506) in comparison to non-teaching hospitals. Secondary outcomes showed that patients in teaching hospitals had higher incidence of septic shock (16.06% vs. 12.53%, P < 0.0001), intensive care unit (ICU) admissions (6.61% vs. 5.07%, P = 0.0002), and intubation (5.30% vs. 3.46%, P < 0.0001) in comparison to non-teaching hospitals.</p><p><strong>Conclusion: </strong>Our study found higher mortality rates for AC patients in teaching hospitals compared to non-teaching hospitals. Teaching hospitals also had higher rates of septic shock, ICU admission, and intubation, with no difference in endoscopic retrograde cholangiopancreatography (ERCP) use. These differences could be due to several factors, such as greater resident and fellow autonomy in teaching hospitals and a potentially more proactive approach by physicians in non-teaching hospitals. Additionally, teaching hospitals often manage more complex, higher-acuity cases, which could contribute to worse outcomes.</p>\",\"PeriodicalId\":12461,\"journal\":{\"name\":\"Gastroenterology Research\",\"volume\":\"18 3\",\"pages\":\"129-138\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151124/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gastroenterology Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/gr2038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr2038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/4 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Impact of Hospital Teaching Status on Outcomes of Acute Cholangitis: A Propensity-Matched Analysis of Hospitalizations in the United States.
Background: Acute cholangitis (AC) is a serious condition caused by partial or complete obstruction of the common bile duct (CBD), leading to biliary tract infection. We aimed to evaluate whether teaching hospitals with trainees and non-teaching hospitals impact the outcome of AC in the United States.
Methods: This study utilized the National Inpatient Sample database to analyze adult hospitalizations (> 18 years old) with a primary diagnosis of AC in the USA from 2016 to 2020. A multivariate logistic regression along with Chi-square and t-tests was performed using SAS 9.4 software to analyze inpatient AC-associated mortality, inflation-adjusted total hospitalization costs (THC), and length of stay (LOS) in US teaching and non-teaching hospitals during the study period.
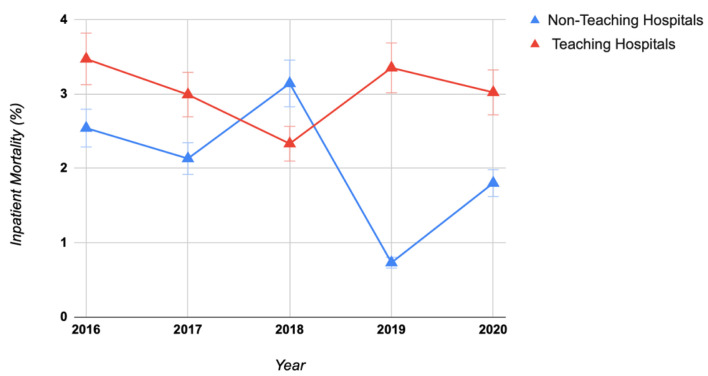
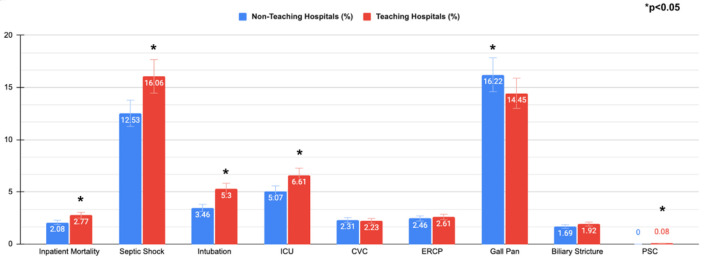
Results: This study included a total of 30,300 patients, out of whom 23,535 (about 78%) were managed in teaching hospitals and 6,765 (about 22%) were managed in non-teaching hospitals. Primary outcomes showed a significant increase in mortality for patients managed in teaching hospitals (2.77% vs. 2.08%, P = 0.01) in comparison to non-teaching hospitals, hospital LOS was slightly higher in teaching hospitals (5 days (interquartile range (IQR): 3 - 6) vs. 4 days (IQR: 3 - 8)) and so did hospital cost ($15,259 vs. $14,506) in comparison to non-teaching hospitals. Secondary outcomes showed that patients in teaching hospitals had higher incidence of septic shock (16.06% vs. 12.53%, P < 0.0001), intensive care unit (ICU) admissions (6.61% vs. 5.07%, P = 0.0002), and intubation (5.30% vs. 3.46%, P < 0.0001) in comparison to non-teaching hospitals.
Conclusion: Our study found higher mortality rates for AC patients in teaching hospitals compared to non-teaching hospitals. Teaching hospitals also had higher rates of septic shock, ICU admission, and intubation, with no difference in endoscopic retrograde cholangiopancreatography (ERCP) use. These differences could be due to several factors, such as greater resident and fellow autonomy in teaching hospitals and a potentially more proactive approach by physicians in non-teaching hospitals. Additionally, teaching hospitals often manage more complex, higher-acuity cases, which could contribute to worse outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


