Tae-Gyun Lee, Duck-Woo Kim, Hong-Min Ahn, Hye-Rim Shin, Mi Jeong Choi, Min Hyeong Jo, Heung-Kwon Oh, Sung-Bum Kang
{"title":"基于新辅助放化疗对中/低位直肠癌淋巴结反应的侧盆腔淋巴结清扫:一项回顾性比较队列研究。","authors":"Tae-Gyun Lee, Duck-Woo Kim, Hong-Min Ahn, Hye-Rim Shin, Mi Jeong Choi, Min Hyeong Jo, Heung-Kwon Oh, Sung-Bum Kang","doi":"10.4174/astr.2025.108.6.333","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Total mesorectal excision (TME) without lateral pelvic lymph node (LPN) dissection (LPND) is feasible in patients with mid/low rectal cancer showing a reduction in LPN size to ≤5 mm following neoadjuvant chemoradiotherapy (nCRT). We aimed to evaluate the clinical outcomes of selective LPNDs based on these criteria.</p><p><strong>Methods: </strong>Patients with mid/low rectal cancer and LPNs >5 mm before nCRT were included and classified based on nCRT response (post-nCRT LPN size ≤5 mm [responsive] <i>vs.</i> >5 mm [persistent]) and surgical procedure (TME alone <i>vs.</i> TME + LPND). In the responsive group, LPND was selectively performed only if morphologic predictors of LPN metastasis were present. Clinical outcomes were analyzed across subgroups.</p><p><strong>Results: </strong>Of 122 patients, 82 were in the responsive group. Within this group, 61 underwent TME alone and 21 underwent TME + LPND. No locoregional recurrence was observed in either subgroup of the responsive group, with similar systemic metastasis rates (13.1% <i>vs.</i> 14.3%, P > 0.99). The TME alone subgroup showed significantly smaller post-nCRT LPN sizes (1.7 ± 2.1 mm <i>vs.</i> 3.9 ± 1.8 mm, P < 0.001) and lower ycN positivity rates (31.1% <i>vs.</i> 71.4%, P = 0.001).</p><p><strong>Conclusion: </strong>Selective LPND based on post-nCRT LPN size ≤5 mm and the absence of morphologic predictors of metastasis may serve as a feasible option for managing mid/low rectal cancer with enlarged LPNs, thereby optimizing local control and reducing unnecessary surgeries.</p>","PeriodicalId":8071,"journal":{"name":"Annals of Surgical Treatment and Research","volume":"108 6","pages":"333-344"},"PeriodicalIF":1.6000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149989/pdf/","citationCount":"0","resultStr":"{\"title\":\"Lateral pelvic lymph node dissection based on nodal response to neoadjuvant chemoradiotherapy in mid/low rectal cancer: a retrospective comparative cohort study.\",\"authors\":\"Tae-Gyun Lee, Duck-Woo Kim, Hong-Min Ahn, Hye-Rim Shin, Mi Jeong Choi, Min Hyeong Jo, Heung-Kwon Oh, Sung-Bum Kang\",\"doi\":\"10.4174/astr.2025.108.6.333\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Total mesorectal excision (TME) without lateral pelvic lymph node (LPN) dissection (LPND) is feasible in patients with mid/low rectal cancer showing a reduction in LPN size to ≤5 mm following neoadjuvant chemoradiotherapy (nCRT). We aimed to evaluate the clinical outcomes of selective LPNDs based on these criteria.</p><p><strong>Methods: </strong>Patients with mid/low rectal cancer and LPNs >5 mm before nCRT were included and classified based on nCRT response (post-nCRT LPN size ≤5 mm [responsive] <i>vs.</i> >5 mm [persistent]) and surgical procedure (TME alone <i>vs.</i> TME + LPND). In the responsive group, LPND was selectively performed only if morphologic predictors of LPN metastasis were present. Clinical outcomes were analyzed across subgroups.</p><p><strong>Results: </strong>Of 122 patients, 82 were in the responsive group. Within this group, 61 underwent TME alone and 21 underwent TME + LPND. No locoregional recurrence was observed in either subgroup of the responsive group, with similar systemic metastasis rates (13.1% <i>vs.</i> 14.3%, P > 0.99). The TME alone subgroup showed significantly smaller post-nCRT LPN sizes (1.7 ± 2.1 mm <i>vs.</i> 3.9 ± 1.8 mm, P < 0.001) and lower ycN positivity rates (31.1% <i>vs.</i> 71.4%, P = 0.001).</p><p><strong>Conclusion: </strong>Selective LPND based on post-nCRT LPN size ≤5 mm and the absence of morphologic predictors of metastasis may serve as a feasible option for managing mid/low rectal cancer with enlarged LPNs, thereby optimizing local control and reducing unnecessary surgeries.</p>\",\"PeriodicalId\":8071,\"journal\":{\"name\":\"Annals of Surgical Treatment and Research\",\"volume\":\"108 6\",\"pages\":\"333-344\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12149989/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Surgical Treatment and Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4174/astr.2025.108.6.333\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Surgical Treatment and Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4174/astr.2025.108.6.333","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/2 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
摘要
目的:对于新辅助放化疗(nCRT)后盆腔外侧淋巴结(LPN)缩小至≤5mm的中/低位直肠癌患者,全肠系膜切除(TME)而不切除盆腔外侧淋巴结(LPN) (LPN) (lnd)是可行的。我们的目的是根据这些标准评估选择性lnnd的临床结果。方法:纳入nCRT前中低位直肠癌伴lppn >5 mm的患者,并根据nCRT反应(nCRT后LPN大小≤5 mm[反应性]vs >5 mm[持续性])和手术方式(TME单独vs TME + LPND)进行分类。在反应组中,只有当LPN转移的形态学预测因素存在时,才选择性地进行LPN手术。对各亚组的临床结果进行分析。结果:122例患者中82例为应答组。本组单独TME 61例,TME + lpd 21例。两组患者均未见局部复发,全身转移率相似(13.1% vs 14.3%, P < 0.99)。单纯TME亚组ncrt后LPN大小(1.7±2.1 mm vs. 3.9±1.8 mm, P < 0.001)和ycN阳性率(31.1% vs. 71.4%, P = 0.001)明显减小。结论:基于ncrt后LPN大小≤5mm和无转移形态学预测因素的选择性LPN可能是治疗LPN扩大的中/低位直肠癌的可行选择,从而优化局部控制并减少不必要的手术。
Lateral pelvic lymph node dissection based on nodal response to neoadjuvant chemoradiotherapy in mid/low rectal cancer: a retrospective comparative cohort study.
Purpose: Total mesorectal excision (TME) without lateral pelvic lymph node (LPN) dissection (LPND) is feasible in patients with mid/low rectal cancer showing a reduction in LPN size to ≤5 mm following neoadjuvant chemoradiotherapy (nCRT). We aimed to evaluate the clinical outcomes of selective LPNDs based on these criteria.
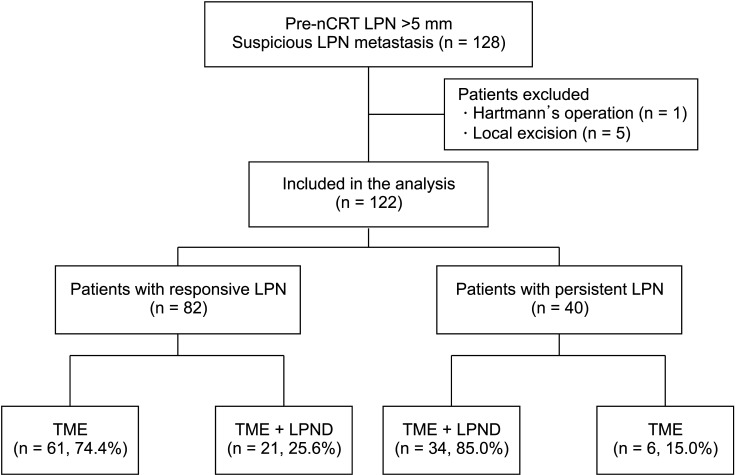
Methods: Patients with mid/low rectal cancer and LPNs >5 mm before nCRT were included and classified based on nCRT response (post-nCRT LPN size ≤5 mm [responsive] vs. >5 mm [persistent]) and surgical procedure (TME alone vs. TME + LPND). In the responsive group, LPND was selectively performed only if morphologic predictors of LPN metastasis were present. Clinical outcomes were analyzed across subgroups.
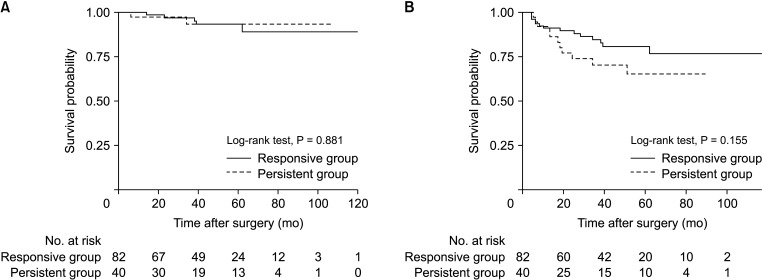
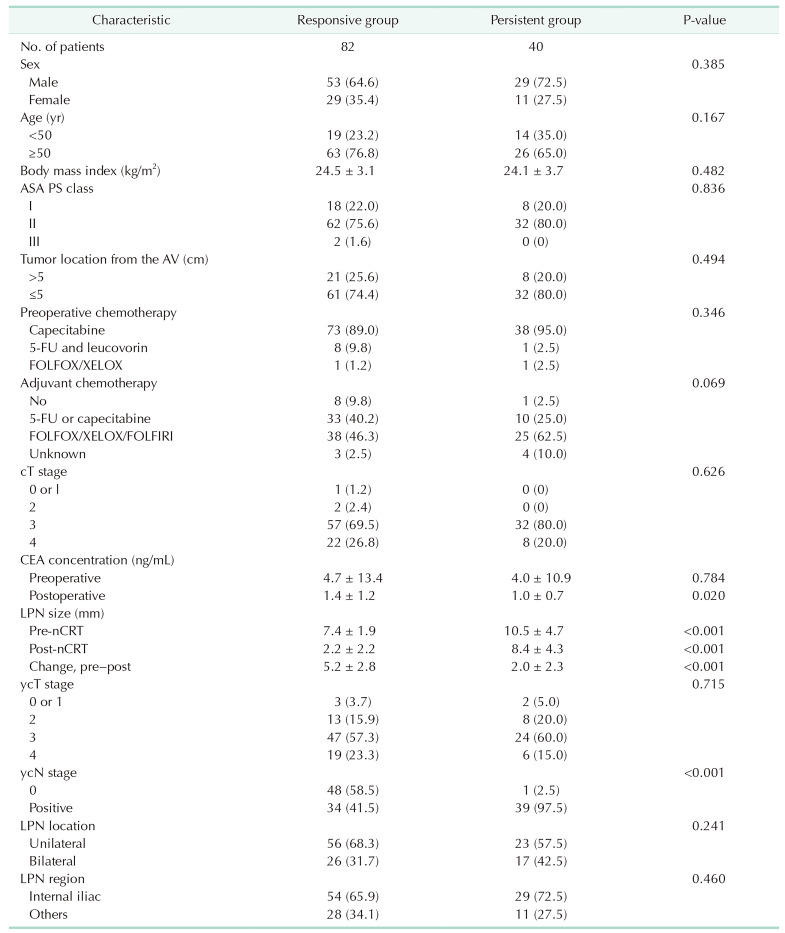
Results: Of 122 patients, 82 were in the responsive group. Within this group, 61 underwent TME alone and 21 underwent TME + LPND. No locoregional recurrence was observed in either subgroup of the responsive group, with similar systemic metastasis rates (13.1% vs. 14.3%, P > 0.99). The TME alone subgroup showed significantly smaller post-nCRT LPN sizes (1.7 ± 2.1 mm vs. 3.9 ± 1.8 mm, P < 0.001) and lower ycN positivity rates (31.1% vs. 71.4%, P = 0.001).
Conclusion: Selective LPND based on post-nCRT LPN size ≤5 mm and the absence of morphologic predictors of metastasis may serve as a feasible option for managing mid/low rectal cancer with enlarged LPNs, thereby optimizing local control and reducing unnecessary surgeries.
期刊介绍:
Manuscripts to the Annals of Surgical Treatment and Research (Ann Surg Treat Res) should be written in English according to the instructions for authors. If the details are not described below, the style should follow the Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publications available at International Committee of Medical Journal Editors (ICMJE) website (http://www.icmje.org).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


