Nicholas Seidler, Shyamal R Asher, Tzonghuei Chen, Paul Gordon, Neel Sodha, Andrew Maslow
{"title":"经导管二尖瓣边缘修复术后因血胸引起的低压填塞。","authors":"Nicholas Seidler, Shyamal R Asher, Tzonghuei Chen, Paul Gordon, Neel Sodha, Andrew Maslow","doi":"10.4330/wjc.v17.i5.106567","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The use of percutaneous transcatheter edge-to-edge repair (TEER) for mitral regurgitation (MR) has increased, including an increased application to older, frailer, and higher risk patients.</p><p><strong>Case summary: </strong>A 74 year-old woman with severe MR, a left ventricular ejection fraction of 45%, and a small circumferential pericardial effusion underwent TEER of the mitral valve. After the placement of two MitraClips, the MR was assessed as mild to moderate. Within 10-20 minutes after the completion of the case, the patient was dyspneic and hypotensive despite volume resuscitation. Point-of-care ultrasound (POCUS) showed no changes in cardiac contractility, valve function, or the pericardial space. The right heart chambers appeared small with right atrial (RA) diastolic collapse. There was no evidence of venous congestion. Further exam showed a large right pleural fluid collection. Given the clinical scenario of dyspnea, hypotension, and diastolic RA collapse, low-pressure tamponade was suspected. A thoracentesis expelled 1200 mL of blood with immediate hemodynamic improvement. The patient made an uneventful recovery.</p><p><strong>Conclusion: </strong>The application of POCUS is crucial for detecting, diagnosing, and properly managing cardiac dysfunction and procedural complications associated with TEER. While tamponade is classically associated with a pericardial effusion and vena caval plethora, their absence does not dismiss the suspicion or diagnosis of tamponade. This case highlights the value of POCUS in assessing low-pressure tamponade caused by a large, pressurized pleural effusion. Clinical suspicion, supported by POCUS findings, was confirmed by a thoracentesis that resulted in immediate hemodynamic improvement.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 5","pages":"106567"},"PeriodicalIF":2.8000,"publicationDate":"2025-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12146957/pdf/","citationCount":"0","resultStr":"{\"title\":\"Low-pressure tamponade due to hemothorax after transcatheter edge-to-edge repair of the mitral valve.\",\"authors\":\"Nicholas Seidler, Shyamal R Asher, Tzonghuei Chen, Paul Gordon, Neel Sodha, Andrew Maslow\",\"doi\":\"10.4330/wjc.v17.i5.106567\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The use of percutaneous transcatheter edge-to-edge repair (TEER) for mitral regurgitation (MR) has increased, including an increased application to older, frailer, and higher risk patients.</p><p><strong>Case summary: </strong>A 74 year-old woman with severe MR, a left ventricular ejection fraction of 45%, and a small circumferential pericardial effusion underwent TEER of the mitral valve. After the placement of two MitraClips, the MR was assessed as mild to moderate. Within 10-20 minutes after the completion of the case, the patient was dyspneic and hypotensive despite volume resuscitation. Point-of-care ultrasound (POCUS) showed no changes in cardiac contractility, valve function, or the pericardial space. The right heart chambers appeared small with right atrial (RA) diastolic collapse. There was no evidence of venous congestion. Further exam showed a large right pleural fluid collection. Given the clinical scenario of dyspnea, hypotension, and diastolic RA collapse, low-pressure tamponade was suspected. A thoracentesis expelled 1200 mL of blood with immediate hemodynamic improvement. The patient made an uneventful recovery.</p><p><strong>Conclusion: </strong>The application of POCUS is crucial for detecting, diagnosing, and properly managing cardiac dysfunction and procedural complications associated with TEER. While tamponade is classically associated with a pericardial effusion and vena caval plethora, their absence does not dismiss the suspicion or diagnosis of tamponade. This case highlights the value of POCUS in assessing low-pressure tamponade caused by a large, pressurized pleural effusion. Clinical suspicion, supported by POCUS findings, was confirmed by a thoracentesis that resulted in immediate hemodynamic improvement.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":\"17 5\",\"pages\":\"106567\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-05-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12146957/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v17.i5.106567\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i5.106567","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Low-pressure tamponade due to hemothorax after transcatheter edge-to-edge repair of the mitral valve.
Background: The use of percutaneous transcatheter edge-to-edge repair (TEER) for mitral regurgitation (MR) has increased, including an increased application to older, frailer, and higher risk patients.
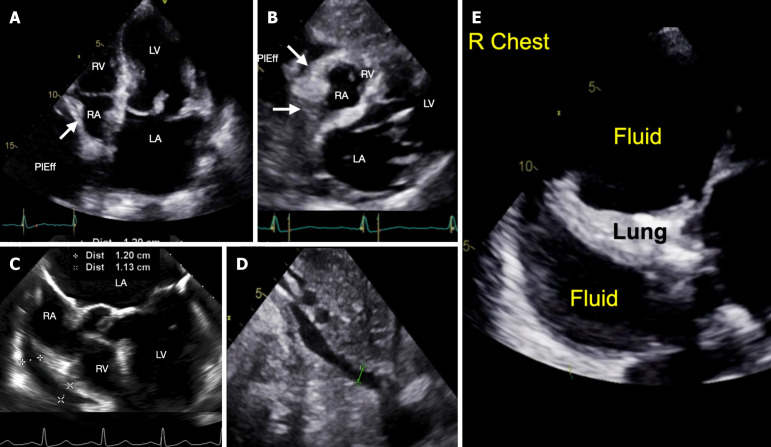
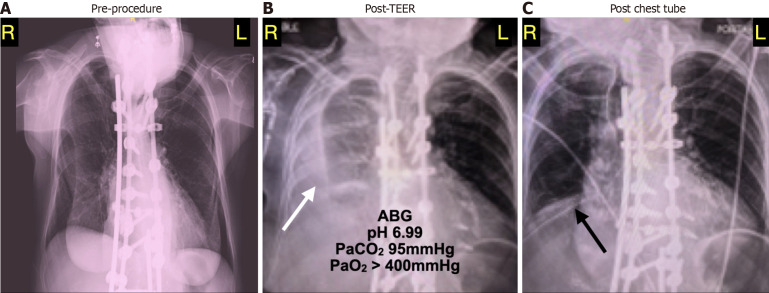
Case summary: A 74 year-old woman with severe MR, a left ventricular ejection fraction of 45%, and a small circumferential pericardial effusion underwent TEER of the mitral valve. After the placement of two MitraClips, the MR was assessed as mild to moderate. Within 10-20 minutes after the completion of the case, the patient was dyspneic and hypotensive despite volume resuscitation. Point-of-care ultrasound (POCUS) showed no changes in cardiac contractility, valve function, or the pericardial space. The right heart chambers appeared small with right atrial (RA) diastolic collapse. There was no evidence of venous congestion. Further exam showed a large right pleural fluid collection. Given the clinical scenario of dyspnea, hypotension, and diastolic RA collapse, low-pressure tamponade was suspected. A thoracentesis expelled 1200 mL of blood with immediate hemodynamic improvement. The patient made an uneventful recovery.
Conclusion: The application of POCUS is crucial for detecting, diagnosing, and properly managing cardiac dysfunction and procedural complications associated with TEER. While tamponade is classically associated with a pericardial effusion and vena caval plethora, their absence does not dismiss the suspicion or diagnosis of tamponade. This case highlights the value of POCUS in assessing low-pressure tamponade caused by a large, pressurized pleural effusion. Clinical suspicion, supported by POCUS findings, was confirmed by a thoracentesis that resulted in immediate hemodynamic improvement.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


