Isabel Emmerick, Hayley Reddington, Tanmay N Patil, Alexander Neamtu, Jiddu Guart, Rebecca Foley, Allison Crawford, Karl Uy, Mark W Maxfield, Yury Rabotnikov, William Phillips, Feiran Lou
{"title":"微创肺切除术后慢性阿片类药物使用的相关因素。","authors":"Isabel Emmerick, Hayley Reddington, Tanmay N Patil, Alexander Neamtu, Jiddu Guart, Rebecca Foley, Allison Crawford, Karl Uy, Mark W Maxfield, Yury Rabotnikov, William Phillips, Feiran Lou","doi":"10.1371/journal.pone.0325354","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Individuals undergoing lung resections experience persistent postoperative pain and are at high risk of chronic postoperative opioid use. This study aims to identify factors associated with chronic opioid use after minimally invasive lung resections (MILR).</p><p><strong>Study design: </strong>This is a retrospective cohort study of individuals who underwent MILR from March 2019 to May 2022 at a single academic institution. The primary outcome was chronic opioid usage, defined as use at least 30 days after surgery. Postoperative pain was managed with a standardized multi-modal pain-control regimen utilizing opioids only as needed. Prescription patterns and dispensing data of opioids at 30-, 60-, and 90-days postoperatively informed usage. Univariate analysis and multivariable logistic regressions (MVLR) were performed.</p><p><strong>Results: </strong>376 patients were included, 38.6% male, 88.8% white, and a mean age of 64.6 years. A total of 248 (66%) underwent anatomical lung resections. 16.5% used opioids at 30 days, 10.1% at 60 days, and 8.5% at 90 days. In the multivariable model, morphine milligram equivalents (MMEs) of opioids on the day before discharge showed a statistically significant association with chronic opioid usage. Age, sex, length of stay, and surgery type were not associated. A 10-unit increase in MMEs increased odds of use at 30-days by 21% (OR 1.21, 95%CI 1.11-1.32, p < 0.001), 20% at 60-days (OR 1.20, 95%CI 1.09 1.32, p < 0.001) and 18% at 90-days (OR 1.18, 95%CI 1.06-1.30, p = 0.002).</p><p><strong>Conclusion: </strong>Higher pre-discharge MMEs are associated with an increased likelihood of chronic opioid usage. Future studies should focus on whether preemptive early outpatient intercostal nerve blocks or cryoablations can decrease chronic narcotic usage in high-risk patients.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 6","pages":"e0325354"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151345/pdf/","citationCount":"0","resultStr":"{\"title\":\"Factors associated with chronic opioid use after minimally invasive lung resections.\",\"authors\":\"Isabel Emmerick, Hayley Reddington, Tanmay N Patil, Alexander Neamtu, Jiddu Guart, Rebecca Foley, Allison Crawford, Karl Uy, Mark W Maxfield, Yury Rabotnikov, William Phillips, Feiran Lou\",\"doi\":\"10.1371/journal.pone.0325354\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Individuals undergoing lung resections experience persistent postoperative pain and are at high risk of chronic postoperative opioid use. This study aims to identify factors associated with chronic opioid use after minimally invasive lung resections (MILR).</p><p><strong>Study design: </strong>This is a retrospective cohort study of individuals who underwent MILR from March 2019 to May 2022 at a single academic institution. The primary outcome was chronic opioid usage, defined as use at least 30 days after surgery. Postoperative pain was managed with a standardized multi-modal pain-control regimen utilizing opioids only as needed. Prescription patterns and dispensing data of opioids at 30-, 60-, and 90-days postoperatively informed usage. Univariate analysis and multivariable logistic regressions (MVLR) were performed.</p><p><strong>Results: </strong>376 patients were included, 38.6% male, 88.8% white, and a mean age of 64.6 years. A total of 248 (66%) underwent anatomical lung resections. 16.5% used opioids at 30 days, 10.1% at 60 days, and 8.5% at 90 days. In the multivariable model, morphine milligram equivalents (MMEs) of opioids on the day before discharge showed a statistically significant association with chronic opioid usage. Age, sex, length of stay, and surgery type were not associated. A 10-unit increase in MMEs increased odds of use at 30-days by 21% (OR 1.21, 95%CI 1.11-1.32, p < 0.001), 20% at 60-days (OR 1.20, 95%CI 1.09 1.32, p < 0.001) and 18% at 90-days (OR 1.18, 95%CI 1.06-1.30, p = 0.002).</p><p><strong>Conclusion: </strong>Higher pre-discharge MMEs are associated with an increased likelihood of chronic opioid usage. Future studies should focus on whether preemptive early outpatient intercostal nerve blocks or cryoablations can decrease chronic narcotic usage in high-risk patients.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 6\",\"pages\":\"e0325354\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-06-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151345/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0325354\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0325354","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Factors associated with chronic opioid use after minimally invasive lung resections.
Background: Individuals undergoing lung resections experience persistent postoperative pain and are at high risk of chronic postoperative opioid use. This study aims to identify factors associated with chronic opioid use after minimally invasive lung resections (MILR).
Study design: This is a retrospective cohort study of individuals who underwent MILR from March 2019 to May 2022 at a single academic institution. The primary outcome was chronic opioid usage, defined as use at least 30 days after surgery. Postoperative pain was managed with a standardized multi-modal pain-control regimen utilizing opioids only as needed. Prescription patterns and dispensing data of opioids at 30-, 60-, and 90-days postoperatively informed usage. Univariate analysis and multivariable logistic regressions (MVLR) were performed.
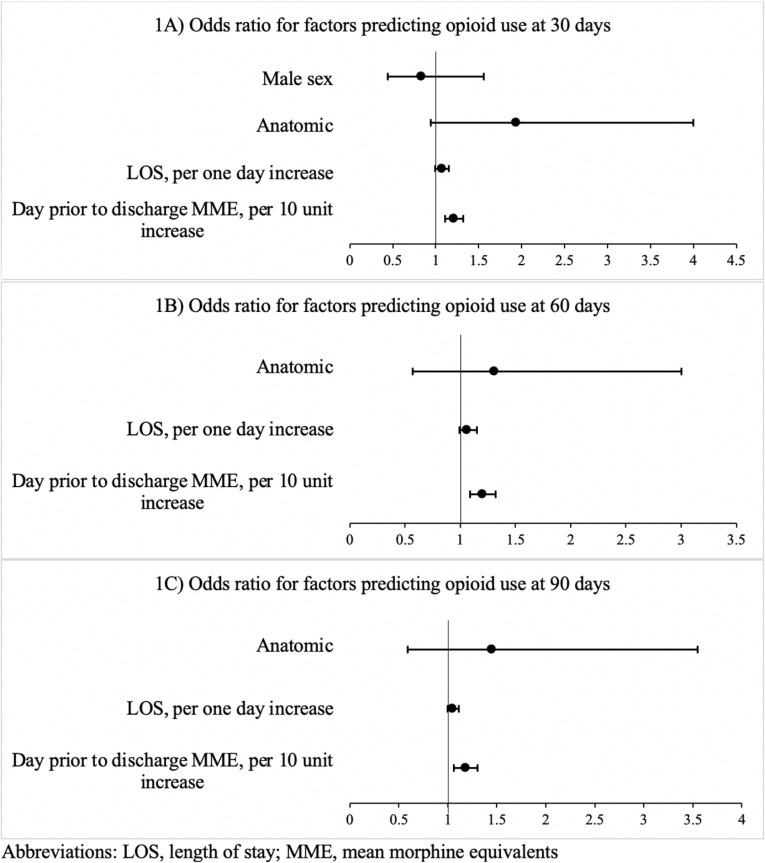
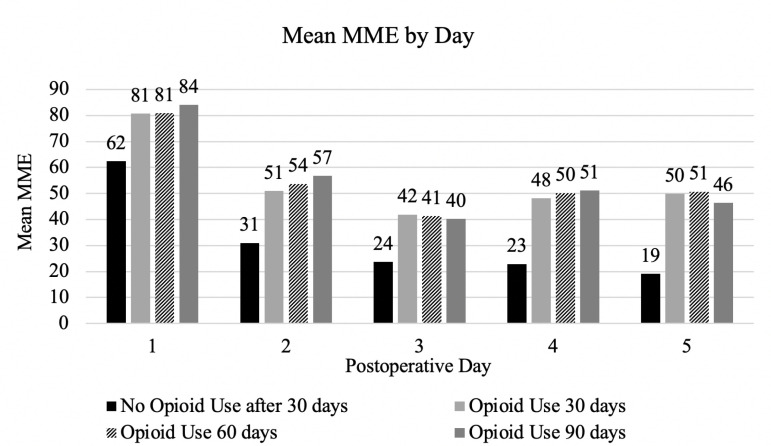
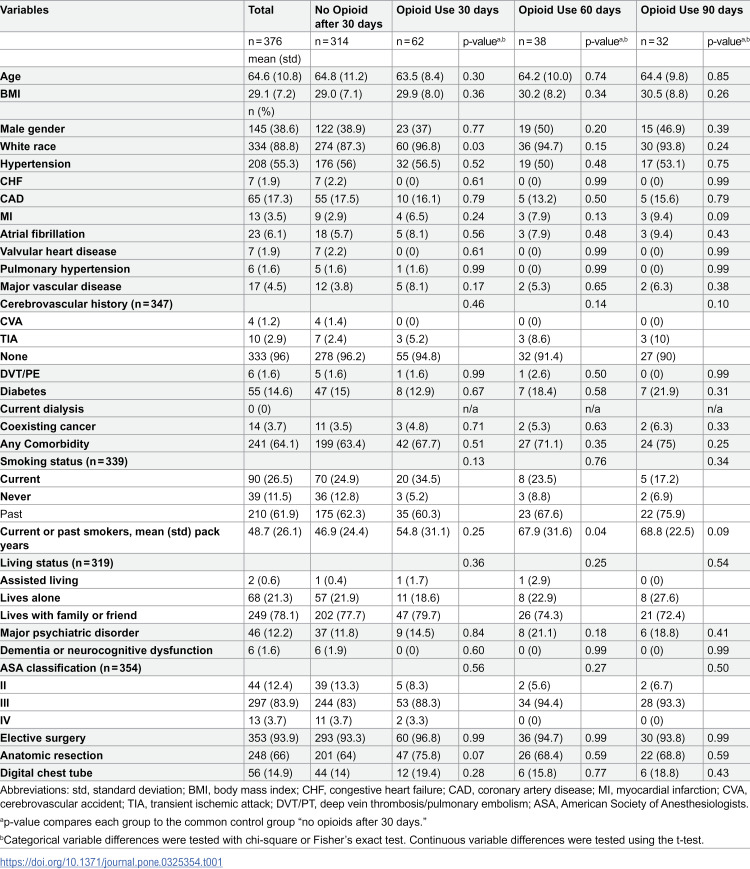
Results: 376 patients were included, 38.6% male, 88.8% white, and a mean age of 64.6 years. A total of 248 (66%) underwent anatomical lung resections. 16.5% used opioids at 30 days, 10.1% at 60 days, and 8.5% at 90 days. In the multivariable model, morphine milligram equivalents (MMEs) of opioids on the day before discharge showed a statistically significant association with chronic opioid usage. Age, sex, length of stay, and surgery type were not associated. A 10-unit increase in MMEs increased odds of use at 30-days by 21% (OR 1.21, 95%CI 1.11-1.32, p < 0.001), 20% at 60-days (OR 1.20, 95%CI 1.09 1.32, p < 0.001) and 18% at 90-days (OR 1.18, 95%CI 1.06-1.30, p = 0.002).
Conclusion: Higher pre-discharge MMEs are associated with an increased likelihood of chronic opioid usage. Future studies should focus on whether preemptive early outpatient intercostal nerve blocks or cryoablations can decrease chronic narcotic usage in high-risk patients.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


