Milani Deb-Chatterji, Parnia Aghel, Hans Pinnschmidt, Christina Krüger, Juliane Herm, Julia Layer, Hebun Erdur, Felix J Bode, Christian H Nolte, Tim Magnus
{"title":"活检证实的PACNS:来自大型多中心脑血管炎患者队列的结果。","authors":"Milani Deb-Chatterji, Parnia Aghel, Hans Pinnschmidt, Christina Krüger, Juliane Herm, Julia Layer, Hebun Erdur, Felix J Bode, Christian H Nolte, Tim Magnus","doi":"10.1136/jnnp-2025-335764","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reports of primary angiitis of the central nervous system (PACNS) are mainly restricted to clinically suspected cases, but biopsy-proven ones are rare. Here, we present results from a large multicentre cohort of patients with biopsy-proven PACNS (BP-PACNS). In particular, we provide insights into characteristics and treatment responses of PACNS subtypes.</p><p><strong>Methods: </strong>BP-PACNS patients treated between 1999 and 2021 were analysed. The outcome was assessed by the modified Rankin Scale (mRS). Between-group comparisons were performed by Kruskal-Wallis, χ<sup>2</sup> or Fisher's exact tests.</p><p><strong>Results: </strong>In total, 57 patients were analysed (52% male). Of these, n=37 (65%) had a lymphocytic (L-PACNS), n=9 (16%) an amyloid-beta-related angiitis (ABRA), n=8 (14%) a granulomatous (G-PACNS) and n=3 (5%) a necrotising (N-PACNS) PACNS subtype. At the time of diagnosis, age differed significantly between groups (median age (years) L-PACNS 47, ABRA 64.5, G-PACNS 37, N-PACNS 65; p=0.008). The clinical course was mostly monophasic in L-PACNS and ABRA (65% and 75%, respectively), while relapsing-remitting in G-PACNS (63%). Median mRS at last follow up was 2 (IQR 1.25-4) in the study group. Worst outcome (median mRS 4) and highest mortality (25%) were seen in G-PACNS. Good induction treatment response was achieved in 77% of all BP-PACNS patients but was low in those with G-PACNS (29%).</p><p><strong>Conclusions: </strong>In this large, multicentre series of BP-PACNS patients, G-PACNS had a worse functional outcome, a predominant relapsing-remitting disease and a poorer response to the induction therapy. An optimal first-line treatment regimen for G-PACNS patients should be further examined and established in larger studies to improve the outcome of G-PACNS patients.</p>","PeriodicalId":16418,"journal":{"name":"Journal of Neurology, Neurosurgery, and Psychiatry","volume":" ","pages":"825-831"},"PeriodicalIF":7.5000,"publicationDate":"2025-08-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421100/pdf/","citationCount":"0","resultStr":"{\"title\":\"Biopsy-proven PACNS: results from the large, multicentre cohort of cerebral vasculitis patients.\",\"authors\":\"Milani Deb-Chatterji, Parnia Aghel, Hans Pinnschmidt, Christina Krüger, Juliane Herm, Julia Layer, Hebun Erdur, Felix J Bode, Christian H Nolte, Tim Magnus\",\"doi\":\"10.1136/jnnp-2025-335764\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Reports of primary angiitis of the central nervous system (PACNS) are mainly restricted to clinically suspected cases, but biopsy-proven ones are rare. Here, we present results from a large multicentre cohort of patients with biopsy-proven PACNS (BP-PACNS). In particular, we provide insights into characteristics and treatment responses of PACNS subtypes.</p><p><strong>Methods: </strong>BP-PACNS patients treated between 1999 and 2021 were analysed. The outcome was assessed by the modified Rankin Scale (mRS). Between-group comparisons were performed by Kruskal-Wallis, χ<sup>2</sup> or Fisher's exact tests.</p><p><strong>Results: </strong>In total, 57 patients were analysed (52% male). Of these, n=37 (65%) had a lymphocytic (L-PACNS), n=9 (16%) an amyloid-beta-related angiitis (ABRA), n=8 (14%) a granulomatous (G-PACNS) and n=3 (5%) a necrotising (N-PACNS) PACNS subtype. At the time of diagnosis, age differed significantly between groups (median age (years) L-PACNS 47, ABRA 64.5, G-PACNS 37, N-PACNS 65; p=0.008). The clinical course was mostly monophasic in L-PACNS and ABRA (65% and 75%, respectively), while relapsing-remitting in G-PACNS (63%). Median mRS at last follow up was 2 (IQR 1.25-4) in the study group. Worst outcome (median mRS 4) and highest mortality (25%) were seen in G-PACNS. Good induction treatment response was achieved in 77% of all BP-PACNS patients but was low in those with G-PACNS (29%).</p><p><strong>Conclusions: </strong>In this large, multicentre series of BP-PACNS patients, G-PACNS had a worse functional outcome, a predominant relapsing-remitting disease and a poorer response to the induction therapy. An optimal first-line treatment regimen for G-PACNS patients should be further examined and established in larger studies to improve the outcome of G-PACNS patients.</p>\",\"PeriodicalId\":16418,\"journal\":{\"name\":\"Journal of Neurology, Neurosurgery, and Psychiatry\",\"volume\":\" \",\"pages\":\"825-831\"},\"PeriodicalIF\":7.5000,\"publicationDate\":\"2025-08-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421100/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurology, Neurosurgery, and Psychiatry\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/jnnp-2025-335764\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurology, Neurosurgery, and Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/jnnp-2025-335764","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Biopsy-proven PACNS: results from the large, multicentre cohort of cerebral vasculitis patients.
Background: Reports of primary angiitis of the central nervous system (PACNS) are mainly restricted to clinically suspected cases, but biopsy-proven ones are rare. Here, we present results from a large multicentre cohort of patients with biopsy-proven PACNS (BP-PACNS). In particular, we provide insights into characteristics and treatment responses of PACNS subtypes.
Methods: BP-PACNS patients treated between 1999 and 2021 were analysed. The outcome was assessed by the modified Rankin Scale (mRS). Between-group comparisons were performed by Kruskal-Wallis, χ2 or Fisher's exact tests.
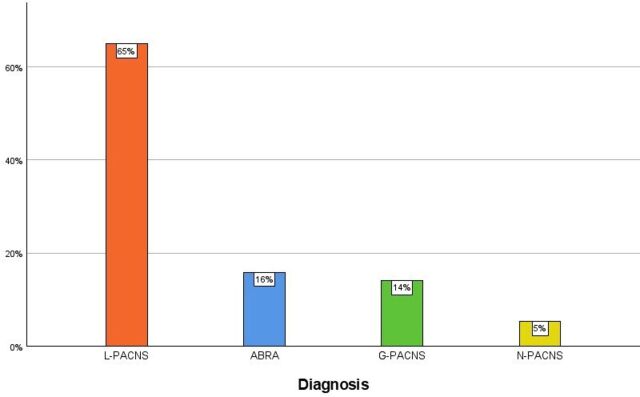
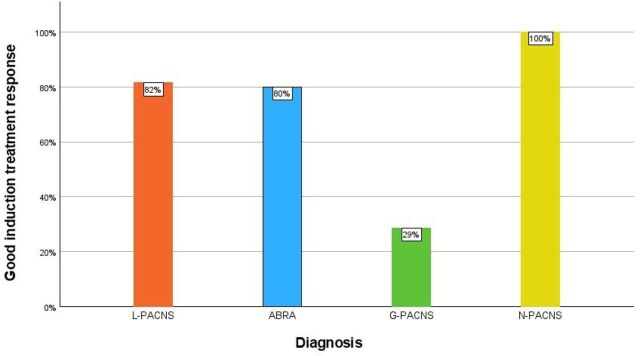
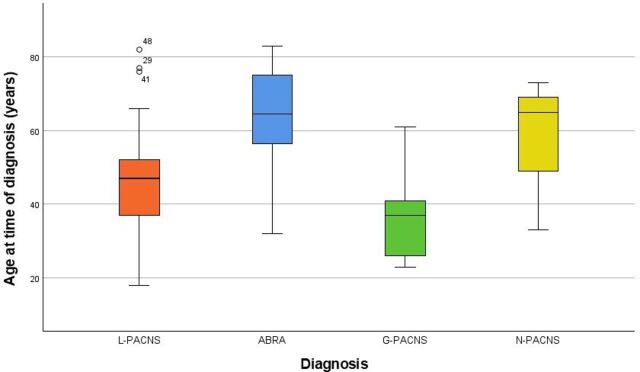
Results: In total, 57 patients were analysed (52% male). Of these, n=37 (65%) had a lymphocytic (L-PACNS), n=9 (16%) an amyloid-beta-related angiitis (ABRA), n=8 (14%) a granulomatous (G-PACNS) and n=3 (5%) a necrotising (N-PACNS) PACNS subtype. At the time of diagnosis, age differed significantly between groups (median age (years) L-PACNS 47, ABRA 64.5, G-PACNS 37, N-PACNS 65; p=0.008). The clinical course was mostly monophasic in L-PACNS and ABRA (65% and 75%, respectively), while relapsing-remitting in G-PACNS (63%). Median mRS at last follow up was 2 (IQR 1.25-4) in the study group. Worst outcome (median mRS 4) and highest mortality (25%) were seen in G-PACNS. Good induction treatment response was achieved in 77% of all BP-PACNS patients but was low in those with G-PACNS (29%).
Conclusions: In this large, multicentre series of BP-PACNS patients, G-PACNS had a worse functional outcome, a predominant relapsing-remitting disease and a poorer response to the induction therapy. An optimal first-line treatment regimen for G-PACNS patients should be further examined and established in larger studies to improve the outcome of G-PACNS patients.
期刊介绍:
The Journal of Neurology, Neurosurgery & Psychiatry (JNNP) aspires to publish groundbreaking and cutting-edge research worldwide. Covering the entire spectrum of neurological sciences, the journal focuses on common disorders like stroke, multiple sclerosis, Parkinson’s disease, epilepsy, peripheral neuropathy, subarachnoid haemorrhage, and neuropsychiatry, while also addressing complex challenges such as ALS. With early online publication, regular podcasts, and an extensive archive collection boasting the longest half-life in clinical neuroscience journals, JNNP aims to be a trailblazer in the field.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


