Georgina Ducker, Ketan Dhatariya, Chetan B Mukhtyar
{"title":"巨细胞动脉炎的肾上腺功能不全。","authors":"Georgina Ducker, Ketan Dhatariya, Chetan B Mukhtyar","doi":"10.1093/rap/rkaf050","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To ascertain the frequency of adrenal insufficiency in patients with GCA treated using the Norwich prednisolone regimen.</p><p><strong>Methods: </strong>Consecutive patients diagnosed with GCA between 1 January 2012 and 31 May 2022 were included. All patients were treated with the Norwich prednisolone regimen, educated about the benefits and risks of long-term prednisolone use and followed up in dedicated vasculitis clinics. When patients contacted the advice line to report being unwell, tests for adrenal function were performed after ruling out relapsing vasculitis or polymyalgia rheumatica. A 9 a.m. serum cortisol was used, providing the daily dose of prednisolone was ≤5 mg, as a gateway to dynamic testing with full-form adrenocorticotrophic hormone (ACTH) stimulation.</p><p><strong>Results: </strong>A total of 353 consecutive patients with GCA were included. During the prescribed glucocorticoid tapering regimen, 76/353 had a 9 a.m. serum cortisol check after ruling out relapsing disease. Of these, 34/76 had a serum cortisol >350 nmol/l (our laboratory cut-off for adequacy of adrenal reserve); 7/76 had a serum cortisol <100 nmol/l, indicative of insufficient adrenal function and 35/76 had a cortisol level of 100-350 nmol/l. Of the 35 patients who went on to have a standard-dose ACTH stimulation test, 27/35 had an adequate result (i.e. >450 nmol/l at 30 min) and 8/35 had an inadequate result. A total of 15/353 patients required long-term steroids because of adrenal insufficiency and 11/15 patients with adrenal insufficiency were female. The median (IQR) cumulative prednisolone dose at the time of testing was 11.53 grams (7.74) and the median (IQR) duration of prednisolone was 121 weeks (97).</p><p><strong>Conclusion: </strong>This is the largest study studying the frequency of adrenal insufficiency in patients with GCA treated using the Norwich prednisolone regimen. Adrenal insufficiency requiring long-term steroid replacement therapy is uncommon. Sequential testing using 9 a.m. serum cortisol levels as a gateway to rationalizing the necessity for dynamic testing with standard-dose ACTH stimulation testing is an efficient strategy for this cohort of patients.</p>","PeriodicalId":21350,"journal":{"name":"Rheumatology Advances in Practice","volume":"9 2","pages":"rkaf050"},"PeriodicalIF":2.1000,"publicationDate":"2025-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12148302/pdf/","citationCount":"0","resultStr":"{\"title\":\"Adrenal insufficiency in giant cell arteritis.\",\"authors\":\"Georgina Ducker, Ketan Dhatariya, Chetan B Mukhtyar\",\"doi\":\"10.1093/rap/rkaf050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To ascertain the frequency of adrenal insufficiency in patients with GCA treated using the Norwich prednisolone regimen.</p><p><strong>Methods: </strong>Consecutive patients diagnosed with GCA between 1 January 2012 and 31 May 2022 were included. All patients were treated with the Norwich prednisolone regimen, educated about the benefits and risks of long-term prednisolone use and followed up in dedicated vasculitis clinics. When patients contacted the advice line to report being unwell, tests for adrenal function were performed after ruling out relapsing vasculitis or polymyalgia rheumatica. A 9 a.m. serum cortisol was used, providing the daily dose of prednisolone was ≤5 mg, as a gateway to dynamic testing with full-form adrenocorticotrophic hormone (ACTH) stimulation.</p><p><strong>Results: </strong>A total of 353 consecutive patients with GCA were included. During the prescribed glucocorticoid tapering regimen, 76/353 had a 9 a.m. serum cortisol check after ruling out relapsing disease. Of these, 34/76 had a serum cortisol >350 nmol/l (our laboratory cut-off for adequacy of adrenal reserve); 7/76 had a serum cortisol <100 nmol/l, indicative of insufficient adrenal function and 35/76 had a cortisol level of 100-350 nmol/l. Of the 35 patients who went on to have a standard-dose ACTH stimulation test, 27/35 had an adequate result (i.e. >450 nmol/l at 30 min) and 8/35 had an inadequate result. A total of 15/353 patients required long-term steroids because of adrenal insufficiency and 11/15 patients with adrenal insufficiency were female. The median (IQR) cumulative prednisolone dose at the time of testing was 11.53 grams (7.74) and the median (IQR) duration of prednisolone was 121 weeks (97).</p><p><strong>Conclusion: </strong>This is the largest study studying the frequency of adrenal insufficiency in patients with GCA treated using the Norwich prednisolone regimen. Adrenal insufficiency requiring long-term steroid replacement therapy is uncommon. Sequential testing using 9 a.m. serum cortisol levels as a gateway to rationalizing the necessity for dynamic testing with standard-dose ACTH stimulation testing is an efficient strategy for this cohort of patients.</p>\",\"PeriodicalId\":21350,\"journal\":{\"name\":\"Rheumatology Advances in Practice\",\"volume\":\"9 2\",\"pages\":\"rkaf050\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-04-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12148302/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rheumatology Advances in Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/rap/rkaf050\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rheumatology Advances in Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/rap/rkaf050","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Objectives: To ascertain the frequency of adrenal insufficiency in patients with GCA treated using the Norwich prednisolone regimen.
Methods: Consecutive patients diagnosed with GCA between 1 January 2012 and 31 May 2022 were included. All patients were treated with the Norwich prednisolone regimen, educated about the benefits and risks of long-term prednisolone use and followed up in dedicated vasculitis clinics. When patients contacted the advice line to report being unwell, tests for adrenal function were performed after ruling out relapsing vasculitis or polymyalgia rheumatica. A 9 a.m. serum cortisol was used, providing the daily dose of prednisolone was ≤5 mg, as a gateway to dynamic testing with full-form adrenocorticotrophic hormone (ACTH) stimulation.
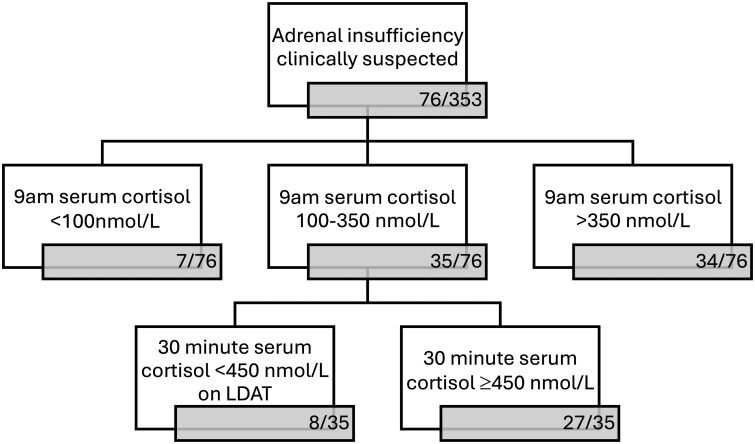
Results: A total of 353 consecutive patients with GCA were included. During the prescribed glucocorticoid tapering regimen, 76/353 had a 9 a.m. serum cortisol check after ruling out relapsing disease. Of these, 34/76 had a serum cortisol >350 nmol/l (our laboratory cut-off for adequacy of adrenal reserve); 7/76 had a serum cortisol <100 nmol/l, indicative of insufficient adrenal function and 35/76 had a cortisol level of 100-350 nmol/l. Of the 35 patients who went on to have a standard-dose ACTH stimulation test, 27/35 had an adequate result (i.e. >450 nmol/l at 30 min) and 8/35 had an inadequate result. A total of 15/353 patients required long-term steroids because of adrenal insufficiency and 11/15 patients with adrenal insufficiency were female. The median (IQR) cumulative prednisolone dose at the time of testing was 11.53 grams (7.74) and the median (IQR) duration of prednisolone was 121 weeks (97).
Conclusion: This is the largest study studying the frequency of adrenal insufficiency in patients with GCA treated using the Norwich prednisolone regimen. Adrenal insufficiency requiring long-term steroid replacement therapy is uncommon. Sequential testing using 9 a.m. serum cortisol levels as a gateway to rationalizing the necessity for dynamic testing with standard-dose ACTH stimulation testing is an efficient strategy for this cohort of patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


