Braeden A Terpou, Lauren Lapointe-Shaw, Ruoxi Wang, Danielle Martin, Mina Tadrous, Sacha Bhatia, Jennifer Shuldiner, Simon Berthelot, Niels Thakkar, Kerry McBrien, Bahram Rahman, Aisha Lofters, J Michael Paterson, Rita McCracken, Christine Salahub, Tara Kiran, Noah M Ivers, Laura Desveaux
{"title":"为简单而设计,为复杂而使用:塑造免预约诊所实践和结果的系统压力。","authors":"Braeden A Terpou, Lauren Lapointe-Shaw, Ruoxi Wang, Danielle Martin, Mina Tadrous, Sacha Bhatia, Jennifer Shuldiner, Simon Berthelot, Niels Thakkar, Kerry McBrien, Bahram Rahman, Aisha Lofters, J Michael Paterson, Rita McCracken, Christine Salahub, Tara Kiran, Noah M Ivers, Laura Desveaux","doi":"10.1371/journal.pone.0325793","DOIUrl":null,"url":null,"abstract":"<p><p>Walk-in clinics (WICs), appreciated for their accessibility and convenience, have become an increasingly popular healthcare option in Ontario for patients with and without primary care enrolment. Despite their utility, WICs face criticism for delivering lower-quality care compared to comprehensive, enrolment-based primary care models. Critics argue that WICs contribute to system inefficiencies and encourage practice patterns misaligned with population health goals. This study explored physician perspectives on two key outcomes often associated with low-quality care in WICs: repeat primary care visits and potentially inappropriate antibiotic prescribing. Using a qualitative descriptive approach, semi-structured interviews were conducted with Ontario-based family physicians (N = 19) who had experience practicing in both WICs and enrolment-based primary care. The findings highlight systemic challenges, including limited access to enrolment-based primary care and increasing healthcare demands, which have pushed WICs beyond their intended role. This misalignment has created tensions between their structure and purpose, resulting in visits that participants described as more transactional than those in primary care. These constraints-rooted in a lack of informational and relational continuity-often limited participants' ability to provide in-depth engagement or follow-up care. Repeat visits were frequently linked to efforts to ensure continuity for complex or chronic conditions. Similarly, participants acknowledged the reality of potentially inappropriate antibiotic prescribing, attributing it to the high patient volume, desire to satisfy patient expectations, and a tendency to \"err on the side of caution\" when the nature of the illness is in question. The findings underscore how health system pressures and well-intended policies, such as Ontario's primary care access bonus, can produce unintended consequences, including inequities in access and difficulties with care coordination across settings. Addressing these challenges requires reforms to better integrate WICs with the primary care system, alongside tailored training to support physician decision-making in episodic care contexts.</p>","PeriodicalId":20189,"journal":{"name":"PLoS ONE","volume":"20 6","pages":"e0325793"},"PeriodicalIF":2.6000,"publicationDate":"2025-06-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12148145/pdf/","citationCount":"0","resultStr":"{\"title\":\"Designed for simplicity, used for complexity: The systemic pressures shaping walk-in clinic practices and outcomes.\",\"authors\":\"Braeden A Terpou, Lauren Lapointe-Shaw, Ruoxi Wang, Danielle Martin, Mina Tadrous, Sacha Bhatia, Jennifer Shuldiner, Simon Berthelot, Niels Thakkar, Kerry McBrien, Bahram Rahman, Aisha Lofters, J Michael Paterson, Rita McCracken, Christine Salahub, Tara Kiran, Noah M Ivers, Laura Desveaux\",\"doi\":\"10.1371/journal.pone.0325793\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Walk-in clinics (WICs), appreciated for their accessibility and convenience, have become an increasingly popular healthcare option in Ontario for patients with and without primary care enrolment. Despite their utility, WICs face criticism for delivering lower-quality care compared to comprehensive, enrolment-based primary care models. Critics argue that WICs contribute to system inefficiencies and encourage practice patterns misaligned with population health goals. This study explored physician perspectives on two key outcomes often associated with low-quality care in WICs: repeat primary care visits and potentially inappropriate antibiotic prescribing. Using a qualitative descriptive approach, semi-structured interviews were conducted with Ontario-based family physicians (N = 19) who had experience practicing in both WICs and enrolment-based primary care. The findings highlight systemic challenges, including limited access to enrolment-based primary care and increasing healthcare demands, which have pushed WICs beyond their intended role. This misalignment has created tensions between their structure and purpose, resulting in visits that participants described as more transactional than those in primary care. These constraints-rooted in a lack of informational and relational continuity-often limited participants' ability to provide in-depth engagement or follow-up care. Repeat visits were frequently linked to efforts to ensure continuity for complex or chronic conditions. Similarly, participants acknowledged the reality of potentially inappropriate antibiotic prescribing, attributing it to the high patient volume, desire to satisfy patient expectations, and a tendency to \\\"err on the side of caution\\\" when the nature of the illness is in question. The findings underscore how health system pressures and well-intended policies, such as Ontario's primary care access bonus, can produce unintended consequences, including inequities in access and difficulties with care coordination across settings. Addressing these challenges requires reforms to better integrate WICs with the primary care system, alongside tailored training to support physician decision-making in episodic care contexts.</p>\",\"PeriodicalId\":20189,\"journal\":{\"name\":\"PLoS ONE\",\"volume\":\"20 6\",\"pages\":\"e0325793\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-06-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12148145/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLoS ONE\",\"FirstCategoryId\":\"103\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pone.0325793\",\"RegionNum\":3,\"RegionCategory\":\"综合性期刊\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS ONE","FirstCategoryId":"103","ListUrlMain":"https://doi.org/10.1371/journal.pone.0325793","RegionNum":3,"RegionCategory":"综合性期刊","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
Designed for simplicity, used for complexity: The systemic pressures shaping walk-in clinic practices and outcomes.
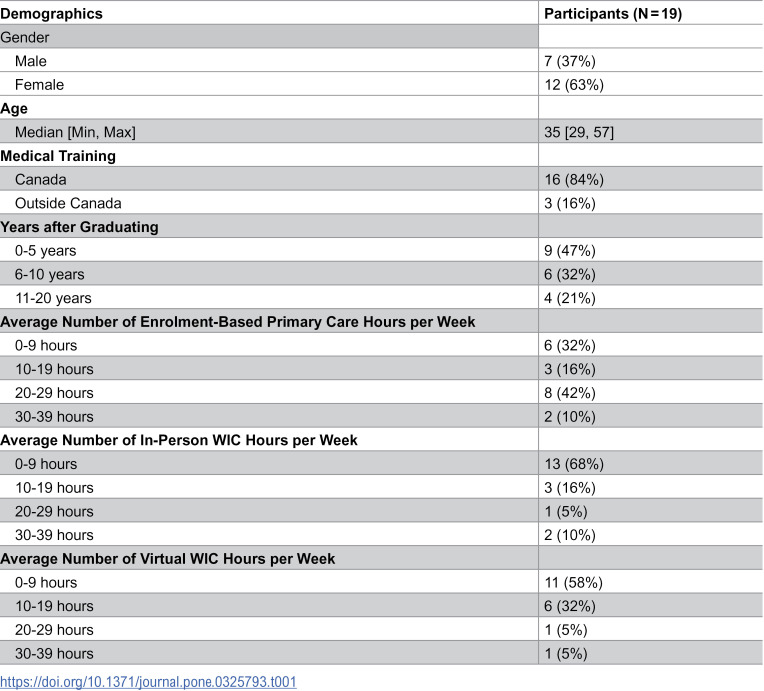
Walk-in clinics (WICs), appreciated for their accessibility and convenience, have become an increasingly popular healthcare option in Ontario for patients with and without primary care enrolment. Despite their utility, WICs face criticism for delivering lower-quality care compared to comprehensive, enrolment-based primary care models. Critics argue that WICs contribute to system inefficiencies and encourage practice patterns misaligned with population health goals. This study explored physician perspectives on two key outcomes often associated with low-quality care in WICs: repeat primary care visits and potentially inappropriate antibiotic prescribing. Using a qualitative descriptive approach, semi-structured interviews were conducted with Ontario-based family physicians (N = 19) who had experience practicing in both WICs and enrolment-based primary care. The findings highlight systemic challenges, including limited access to enrolment-based primary care and increasing healthcare demands, which have pushed WICs beyond their intended role. This misalignment has created tensions between their structure and purpose, resulting in visits that participants described as more transactional than those in primary care. These constraints-rooted in a lack of informational and relational continuity-often limited participants' ability to provide in-depth engagement or follow-up care. Repeat visits were frequently linked to efforts to ensure continuity for complex or chronic conditions. Similarly, participants acknowledged the reality of potentially inappropriate antibiotic prescribing, attributing it to the high patient volume, desire to satisfy patient expectations, and a tendency to "err on the side of caution" when the nature of the illness is in question. The findings underscore how health system pressures and well-intended policies, such as Ontario's primary care access bonus, can produce unintended consequences, including inequities in access and difficulties with care coordination across settings. Addressing these challenges requires reforms to better integrate WICs with the primary care system, alongside tailored training to support physician decision-making in episodic care contexts.
期刊介绍:
PLOS ONE is an international, peer-reviewed, open-access, online publication. PLOS ONE welcomes reports on primary research from any scientific discipline. It provides:
* Open-access—freely accessible online, authors retain copyright
* Fast publication times
* Peer review by expert, practicing researchers
* Post-publication tools to indicate quality and impact
* Community-based dialogue on articles
* Worldwide media coverage

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


