Jeremiah Hwee, Lynn Huynh, Wilson da Costa, Marc E Rothenberg, Mei Sheng Duh, Rafael Alfonso-Cristancho
{"title":"高嗜酸性粒细胞综合征生物使用类固醇的益处和跨亚型的实质性疾病负担。","authors":"Jeremiah Hwee, Lynn Huynh, Wilson da Costa, Marc E Rothenberg, Mei Sheng Duh, Rafael Alfonso-Cristancho","doi":"10.3389/falgy.2025.1605397","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited data exist on the burden of myeloproliferative, lymphocytic and idiopathic subtypes of hypereosinophilic syndrome (M-HES, L-HES and I-HES) and the characteristics of patients with HES receiving biologic therapies. This analysis aimed to further characterize these subtypes and explore the impact of biologics in a real-world European setting.</p><p><strong>Methods: </strong>This was a <i>post hoc</i> subgroup analysis of a retrospective, non-interventional, chart review (GSK ID: 214657) across five European countries. Index date was first clinical visit during January 2015-December 2019 (after or at time of HES diagnosis). Patients with HES aged ≥6 years with ≥1-year follow-up from index were included. Demographics, disease characteristics, diagnostic assessments, comorbidities, types of treatment, clinical manifestations, clinical outcomes and HES-related healthcare resource utilization were summarized for HES overall and subtypes. Oral corticosteroid (OCS) use and clinical manifestations/outcomes were assessed 12-months pre- and post-biologics.</p><p><strong>Results: </strong>The analysis included 280 patients with I-HES (<i>n</i> = 155), M-HES (<i>n</i> = 66), L-HES (<i>n</i> = 42) and chronic eosinophilic leukemia (<i>n</i> = 2). The most common clinical manifestations were fatigue (54.2% I-HES, 52.4% L-HES, 42.4% M-HES), skin itch (36.4% M-HES, 35.7% L-HES, 33.5% I-HES) and pain (31.0% L-HES, 30.3% M-HES, 27.1% I-HES). Biologic use was highest with L-HES (64.3%), followed by I-HES (43.9%) and M-HES (34.8%). Clinical response rates were highest for the I-HES subtype (75.5%; 66.7% L-HES, 63.6% M-HES). Hospitalizations were highest for L-HES (45.2%; 30.3% M-HES, 25.8% I-HES). The annualized rate of OCS prescriptions reduced by 56.8% (0.44-0.19 per person-year) and the proportion of patients with ≥1 clinical response increased 3.6-fold (6.5%-23.4%) between the pre- and post-biologics periods.</p><p><strong>Conclusions: </strong>All HES subtypes had a substantial disease burden and were commonly associated with fatigue, skin itch and pain. I-HES appeared to be more responsive to treatment than L-HES and M-HES. Biologic use for HES led to more patients experiencing clinical responses and was OCS-sparing.</p>","PeriodicalId":73062,"journal":{"name":"Frontiers in allergy","volume":"6 ","pages":"1605397"},"PeriodicalIF":3.1000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143263/pdf/","citationCount":"0","resultStr":"{\"title\":\"Steroid-sparing benefits of biologic use in hypereosinophilic syndrome and substantial disease burden across subtypes.\",\"authors\":\"Jeremiah Hwee, Lynn Huynh, Wilson da Costa, Marc E Rothenberg, Mei Sheng Duh, Rafael Alfonso-Cristancho\",\"doi\":\"10.3389/falgy.2025.1605397\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Limited data exist on the burden of myeloproliferative, lymphocytic and idiopathic subtypes of hypereosinophilic syndrome (M-HES, L-HES and I-HES) and the characteristics of patients with HES receiving biologic therapies. This analysis aimed to further characterize these subtypes and explore the impact of biologics in a real-world European setting.</p><p><strong>Methods: </strong>This was a <i>post hoc</i> subgroup analysis of a retrospective, non-interventional, chart review (GSK ID: 214657) across five European countries. Index date was first clinical visit during January 2015-December 2019 (after or at time of HES diagnosis). Patients with HES aged ≥6 years with ≥1-year follow-up from index were included. Demographics, disease characteristics, diagnostic assessments, comorbidities, types of treatment, clinical manifestations, clinical outcomes and HES-related healthcare resource utilization were summarized for HES overall and subtypes. Oral corticosteroid (OCS) use and clinical manifestations/outcomes were assessed 12-months pre- and post-biologics.</p><p><strong>Results: </strong>The analysis included 280 patients with I-HES (<i>n</i> = 155), M-HES (<i>n</i> = 66), L-HES (<i>n</i> = 42) and chronic eosinophilic leukemia (<i>n</i> = 2). The most common clinical manifestations were fatigue (54.2% I-HES, 52.4% L-HES, 42.4% M-HES), skin itch (36.4% M-HES, 35.7% L-HES, 33.5% I-HES) and pain (31.0% L-HES, 30.3% M-HES, 27.1% I-HES). Biologic use was highest with L-HES (64.3%), followed by I-HES (43.9%) and M-HES (34.8%). Clinical response rates were highest for the I-HES subtype (75.5%; 66.7% L-HES, 63.6% M-HES). Hospitalizations were highest for L-HES (45.2%; 30.3% M-HES, 25.8% I-HES). The annualized rate of OCS prescriptions reduced by 56.8% (0.44-0.19 per person-year) and the proportion of patients with ≥1 clinical response increased 3.6-fold (6.5%-23.4%) between the pre- and post-biologics periods.</p><p><strong>Conclusions: </strong>All HES subtypes had a substantial disease burden and were commonly associated with fatigue, skin itch and pain. I-HES appeared to be more responsive to treatment than L-HES and M-HES. Biologic use for HES led to more patients experiencing clinical responses and was OCS-sparing.</p>\",\"PeriodicalId\":73062,\"journal\":{\"name\":\"Frontiers in allergy\",\"volume\":\"6 \",\"pages\":\"1605397\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143263/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in allergy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/falgy.2025.1605397\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in allergy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/falgy.2025.1605397","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
Steroid-sparing benefits of biologic use in hypereosinophilic syndrome and substantial disease burden across subtypes.
Background: Limited data exist on the burden of myeloproliferative, lymphocytic and idiopathic subtypes of hypereosinophilic syndrome (M-HES, L-HES and I-HES) and the characteristics of patients with HES receiving biologic therapies. This analysis aimed to further characterize these subtypes and explore the impact of biologics in a real-world European setting.
Methods: This was a post hoc subgroup analysis of a retrospective, non-interventional, chart review (GSK ID: 214657) across five European countries. Index date was first clinical visit during January 2015-December 2019 (after or at time of HES diagnosis). Patients with HES aged ≥6 years with ≥1-year follow-up from index were included. Demographics, disease characteristics, diagnostic assessments, comorbidities, types of treatment, clinical manifestations, clinical outcomes and HES-related healthcare resource utilization were summarized for HES overall and subtypes. Oral corticosteroid (OCS) use and clinical manifestations/outcomes were assessed 12-months pre- and post-biologics.
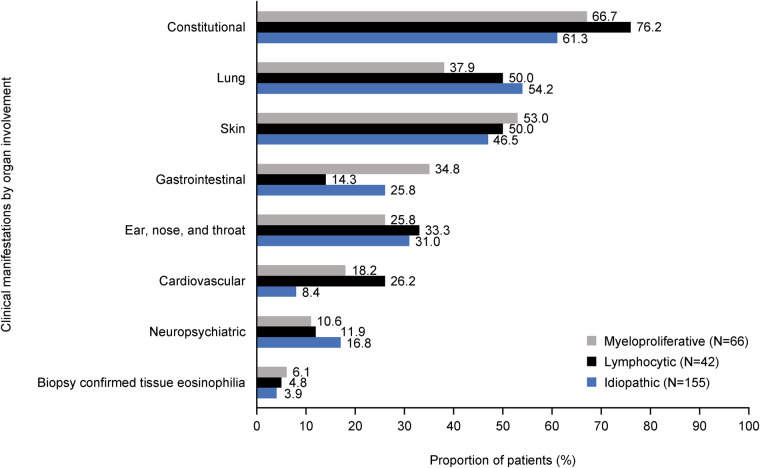
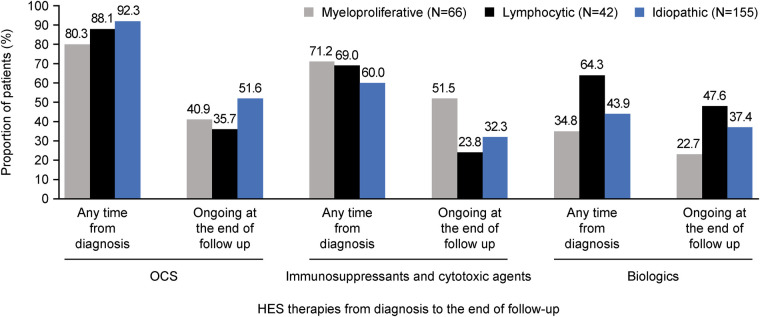
Results: The analysis included 280 patients with I-HES (n = 155), M-HES (n = 66), L-HES (n = 42) and chronic eosinophilic leukemia (n = 2). The most common clinical manifestations were fatigue (54.2% I-HES, 52.4% L-HES, 42.4% M-HES), skin itch (36.4% M-HES, 35.7% L-HES, 33.5% I-HES) and pain (31.0% L-HES, 30.3% M-HES, 27.1% I-HES). Biologic use was highest with L-HES (64.3%), followed by I-HES (43.9%) and M-HES (34.8%). Clinical response rates were highest for the I-HES subtype (75.5%; 66.7% L-HES, 63.6% M-HES). Hospitalizations were highest for L-HES (45.2%; 30.3% M-HES, 25.8% I-HES). The annualized rate of OCS prescriptions reduced by 56.8% (0.44-0.19 per person-year) and the proportion of patients with ≥1 clinical response increased 3.6-fold (6.5%-23.4%) between the pre- and post-biologics periods.
Conclusions: All HES subtypes had a substantial disease burden and were commonly associated with fatigue, skin itch and pain. I-HES appeared to be more responsive to treatment than L-HES and M-HES. Biologic use for HES led to more patients experiencing clinical responses and was OCS-sparing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


