Lianping Ti, Tamara Mihic, Arielle Beauchesne, Cameron Grant, Ingrid Frank, Nooreen Haji, Michael Legal, Stephen Shalansky, Seonaid Nolan
{"title":"对加拿大高风险阿片类药物处方的医院阿片类药物管理计划的评估:中断时间序列分析。","authors":"Lianping Ti, Tamara Mihic, Arielle Beauchesne, Cameron Grant, Ingrid Frank, Nooreen Haji, Michael Legal, Stephen Shalansky, Seonaid Nolan","doi":"10.1186/s13722-025-00574-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-risk opioid prescribing (e.g., high daily dose opioids, concurrent opioid-sedatives) is prevalent in hospitals and linked to adverse outcomes. Opioid stewardship programs (OSP) have the potential to reduce high-risk opioid prescribing through audit-and-feedback recommendations.</p><p><strong>Methods: </strong>We evaluated an audit-and-feedback based OSP implemented in January 2020 at a Vancouver, Canada tertiary care hospital using interrupted time series analysis. An electronic health record (EHR) system with computerized provider order entry (CPOE) was simultaneously operationalized. The main outcome was: any high-risk opioid prescribing (based on 10 evidence-based indicators), including high daily dose of morphine milligram equivalent (MME) prescribing (> 90MME), long opioid prescription duration (> 5 days post-admission), and concurrent opioid-sedative prescribing.</p><p><strong>Results: </strong>Between January 2018 and March 2022, 5,477 active opioid patient encounters were included. While no significant change occurred in overall high-risk opioid prescribing post-OSP (p > 0.05), a significant reduction was seen in the level of high daily dose of MME prescriptions (estimate: -0.044; 95% confidence interval [CI]: -0.082, -0.006). Conversely, the trend in long opioid duration increased (estimate: 0.006; 95%CI: 0.000, 0.011), likely due to the removal of automatic stop dates with the implementation of the EHR with CPOE. Post-OSP intervention, we initially saw an acute increase in concurrent opioid-sedative prescriptions (estimate: 0.013; 95%CI: 0.005, 0.020). A benzodiazepine ordering intervention implemented in May 2021 reversed this trend, reducing both the level (estimate: 0.874; 95%CI: 0.374, 1.375) and slope (estimate: -0.022, 95%CI: -0.034, -0.011) of concurrent prescriptions.</p><p><strong>Conclusion: </strong>The implementation of a new EHR concordant with that of the OSP may have impacted our study's results. While our research suggests the OSP reduced high-dose opioid prescribing, other indicators impacted by the EHR system did not benefit as highly from the OSP. Nevertheless, the OSP proved able to rapidly respond to unintended consequences by introducing interventions to reduce concurrent opioid and sedative prescribing.</p>","PeriodicalId":54223,"journal":{"name":"Addiction Science & Clinical Practice","volume":"20 1","pages":"47"},"PeriodicalIF":3.2000,"publicationDate":"2025-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143091/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluation of a hospital-based opioid stewardship program on high-risk opioid prescribing in a Canadian setting: an interrupted time series analysis.\",\"authors\":\"Lianping Ti, Tamara Mihic, Arielle Beauchesne, Cameron Grant, Ingrid Frank, Nooreen Haji, Michael Legal, Stephen Shalansky, Seonaid Nolan\",\"doi\":\"10.1186/s13722-025-00574-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>High-risk opioid prescribing (e.g., high daily dose opioids, concurrent opioid-sedatives) is prevalent in hospitals and linked to adverse outcomes. Opioid stewardship programs (OSP) have the potential to reduce high-risk opioid prescribing through audit-and-feedback recommendations.</p><p><strong>Methods: </strong>We evaluated an audit-and-feedback based OSP implemented in January 2020 at a Vancouver, Canada tertiary care hospital using interrupted time series analysis. An electronic health record (EHR) system with computerized provider order entry (CPOE) was simultaneously operationalized. The main outcome was: any high-risk opioid prescribing (based on 10 evidence-based indicators), including high daily dose of morphine milligram equivalent (MME) prescribing (> 90MME), long opioid prescription duration (> 5 days post-admission), and concurrent opioid-sedative prescribing.</p><p><strong>Results: </strong>Between January 2018 and March 2022, 5,477 active opioid patient encounters were included. While no significant change occurred in overall high-risk opioid prescribing post-OSP (p > 0.05), a significant reduction was seen in the level of high daily dose of MME prescriptions (estimate: -0.044; 95% confidence interval [CI]: -0.082, -0.006). Conversely, the trend in long opioid duration increased (estimate: 0.006; 95%CI: 0.000, 0.011), likely due to the removal of automatic stop dates with the implementation of the EHR with CPOE. Post-OSP intervention, we initially saw an acute increase in concurrent opioid-sedative prescriptions (estimate: 0.013; 95%CI: 0.005, 0.020). A benzodiazepine ordering intervention implemented in May 2021 reversed this trend, reducing both the level (estimate: 0.874; 95%CI: 0.374, 1.375) and slope (estimate: -0.022, 95%CI: -0.034, -0.011) of concurrent prescriptions.</p><p><strong>Conclusion: </strong>The implementation of a new EHR concordant with that of the OSP may have impacted our study's results. While our research suggests the OSP reduced high-dose opioid prescribing, other indicators impacted by the EHR system did not benefit as highly from the OSP. Nevertheless, the OSP proved able to rapidly respond to unintended consequences by introducing interventions to reduce concurrent opioid and sedative prescribing.</p>\",\"PeriodicalId\":54223,\"journal\":{\"name\":\"Addiction Science & Clinical Practice\",\"volume\":\"20 1\",\"pages\":\"47\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-06-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143091/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Addiction Science & Clinical Practice\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13722-025-00574-x\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SUBSTANCE ABUSE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Addiction Science & Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13722-025-00574-x","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
Evaluation of a hospital-based opioid stewardship program on high-risk opioid prescribing in a Canadian setting: an interrupted time series analysis.
Background: High-risk opioid prescribing (e.g., high daily dose opioids, concurrent opioid-sedatives) is prevalent in hospitals and linked to adverse outcomes. Opioid stewardship programs (OSP) have the potential to reduce high-risk opioid prescribing through audit-and-feedback recommendations.
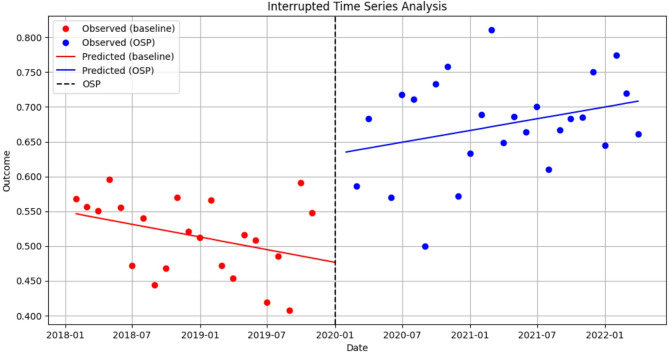
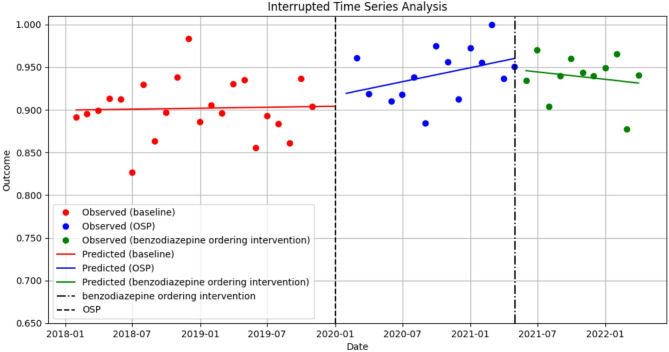
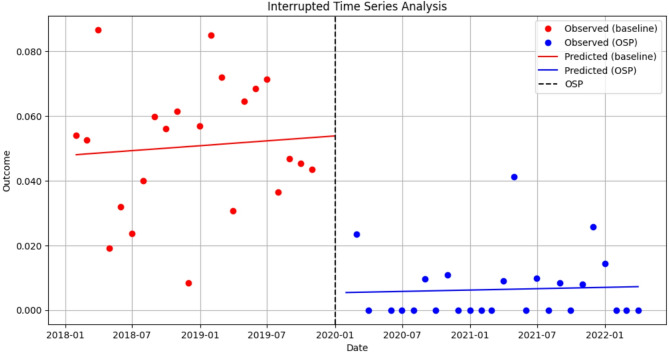
Methods: We evaluated an audit-and-feedback based OSP implemented in January 2020 at a Vancouver, Canada tertiary care hospital using interrupted time series analysis. An electronic health record (EHR) system with computerized provider order entry (CPOE) was simultaneously operationalized. The main outcome was: any high-risk opioid prescribing (based on 10 evidence-based indicators), including high daily dose of morphine milligram equivalent (MME) prescribing (> 90MME), long opioid prescription duration (> 5 days post-admission), and concurrent opioid-sedative prescribing.
Results: Between January 2018 and March 2022, 5,477 active opioid patient encounters were included. While no significant change occurred in overall high-risk opioid prescribing post-OSP (p > 0.05), a significant reduction was seen in the level of high daily dose of MME prescriptions (estimate: -0.044; 95% confidence interval [CI]: -0.082, -0.006). Conversely, the trend in long opioid duration increased (estimate: 0.006; 95%CI: 0.000, 0.011), likely due to the removal of automatic stop dates with the implementation of the EHR with CPOE. Post-OSP intervention, we initially saw an acute increase in concurrent opioid-sedative prescriptions (estimate: 0.013; 95%CI: 0.005, 0.020). A benzodiazepine ordering intervention implemented in May 2021 reversed this trend, reducing both the level (estimate: 0.874; 95%CI: 0.374, 1.375) and slope (estimate: -0.022, 95%CI: -0.034, -0.011) of concurrent prescriptions.
Conclusion: The implementation of a new EHR concordant with that of the OSP may have impacted our study's results. While our research suggests the OSP reduced high-dose opioid prescribing, other indicators impacted by the EHR system did not benefit as highly from the OSP. Nevertheless, the OSP proved able to rapidly respond to unintended consequences by introducing interventions to reduce concurrent opioid and sedative prescribing.
期刊介绍:
Addiction Science & Clinical Practice provides a forum for clinically relevant research and perspectives that contribute to improving the quality of care for people with unhealthy alcohol, tobacco, or other drug use and addictive behaviours across a spectrum of clinical settings.
Addiction Science & Clinical Practice accepts articles of clinical relevance related to the prevention and treatment of unhealthy alcohol, tobacco, and other drug use across the spectrum of clinical settings. Topics of interest address issues related to the following: the spectrum of unhealthy use of alcohol, tobacco, and other drugs among the range of affected persons (e.g., not limited by age, race/ethnicity, gender, or sexual orientation); the array of clinical prevention and treatment practices (from health messages, to identification and early intervention, to more extensive interventions including counseling and pharmacotherapy and other management strategies); and identification and management of medical, psychiatric, social, and other health consequences of substance use.
Addiction Science & Clinical Practice is particularly interested in articles that address how to improve the quality of care for people with unhealthy substance use and related conditions as described in the (US) Institute of Medicine report, Improving the Quality of Healthcare for Mental Health and Substance Use Conditions (Washington, DC: National Academies Press, 2006). Such articles address the quality of care and of health services. Although the journal also welcomes submissions that address these conditions in addiction speciality-treatment settings, the journal is particularly interested in including articles that address unhealthy use outside these settings, including experience with novel models of care and outcomes, and outcomes of research-practice collaborations.
Although Addiction Science & Clinical Practice is generally not an outlet for basic science research, we will accept basic science research manuscripts that have clearly described potential clinical relevance and are accessible to audiences outside a narrow laboratory research field.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


