{"title":"原发性纵隔大b细胞淋巴瘤:一个诊断难题。","authors":"Yazan Alrefai, Shruti Wadhwani, Nikita Wadhwani, Ayrton Bangolo, Jason Mizrahi, Tatyana Feldman","doi":"10.1159/000545931","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Primary mediastinal large B-cell lymphoma (PMBCL) is a rare and aggressive non-Hodgkin lymphoma originating from mediastinal thymic B cells. Its peculiar molecular signature assists in differentiating it from other subtypes of non-Hodgkin lymphoma.</p><p><strong>Case report: </strong>We present a rare case of PMBCL in a 39-year-old male with a bulky mediastinal mass that resulted in superior vena cava thrombosis and cardiac tamponade. Diagnostic discordance between histopathological and molecular data led to a delay in interception of this entity. Histopathology findings were suggestive of spindle-cell neoplasm. Contrastingly, next-generation sequencing (NGS) and immunohistochemistry (IHC) yielded a molecular diagnosis of PMBCL. IHC staining revealed that the atypical cells were positive for CD20, PAX5, CD79a, CD30, CD23, MUM1, and weakly positive for MAL (myelin and lymphocyte) protein. NGS showed increased expression of TNFRSF8 and CD274 genes, which encode CD30 and PDL1 proteins, respectively. The patient was successfully treated with the R-Hyper-CVAD protocol without consolidative radiotherapy.</p><p><strong>Conclusion: </strong>Diagnosing PMBCL can be challenging because it lacks pathognomonic features and shares characteristics with other lymphomas. Molecular testing is of paramount importance in this context owing to its distinctive immunophenotype.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"711-719"},"PeriodicalIF":0.7000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143869/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary Mediastinal Large B-cell Lymphoma: A Diagnostic Conundrum.\",\"authors\":\"Yazan Alrefai, Shruti Wadhwani, Nikita Wadhwani, Ayrton Bangolo, Jason Mizrahi, Tatyana Feldman\",\"doi\":\"10.1159/000545931\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Primary mediastinal large B-cell lymphoma (PMBCL) is a rare and aggressive non-Hodgkin lymphoma originating from mediastinal thymic B cells. Its peculiar molecular signature assists in differentiating it from other subtypes of non-Hodgkin lymphoma.</p><p><strong>Case report: </strong>We present a rare case of PMBCL in a 39-year-old male with a bulky mediastinal mass that resulted in superior vena cava thrombosis and cardiac tamponade. Diagnostic discordance between histopathological and molecular data led to a delay in interception of this entity. Histopathology findings were suggestive of spindle-cell neoplasm. Contrastingly, next-generation sequencing (NGS) and immunohistochemistry (IHC) yielded a molecular diagnosis of PMBCL. IHC staining revealed that the atypical cells were positive for CD20, PAX5, CD79a, CD30, CD23, MUM1, and weakly positive for MAL (myelin and lymphocyte) protein. NGS showed increased expression of TNFRSF8 and CD274 genes, which encode CD30 and PDL1 proteins, respectively. The patient was successfully treated with the R-Hyper-CVAD protocol without consolidative radiotherapy.</p><p><strong>Conclusion: </strong>Diagnosing PMBCL can be challenging because it lacks pathognomonic features and shares characteristics with other lymphomas. Molecular testing is of paramount importance in this context owing to its distinctive immunophenotype.</p>\",\"PeriodicalId\":9625,\"journal\":{\"name\":\"Case Reports in Oncology\",\"volume\":\"18 1\",\"pages\":\"711-719\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12143869/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000545931\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545931","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Primary Mediastinal Large B-cell Lymphoma: A Diagnostic Conundrum.
Introduction: Primary mediastinal large B-cell lymphoma (PMBCL) is a rare and aggressive non-Hodgkin lymphoma originating from mediastinal thymic B cells. Its peculiar molecular signature assists in differentiating it from other subtypes of non-Hodgkin lymphoma.
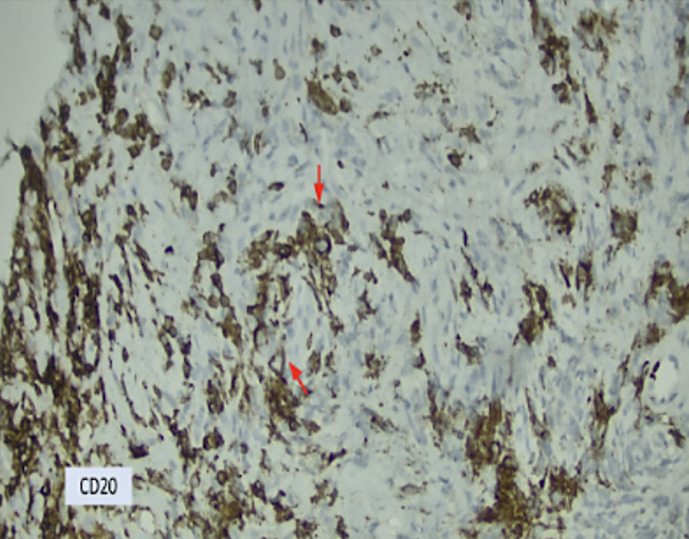
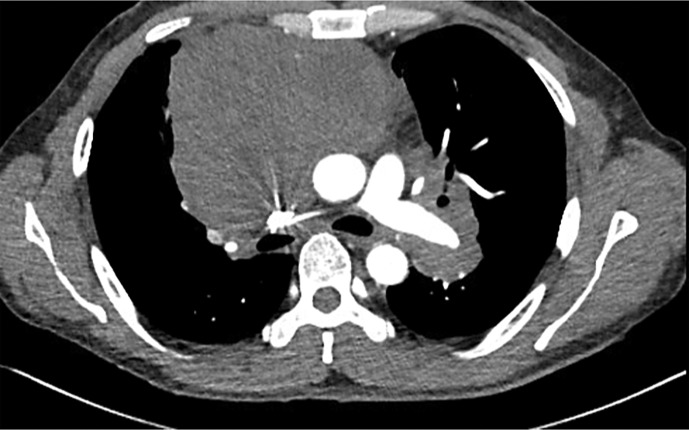
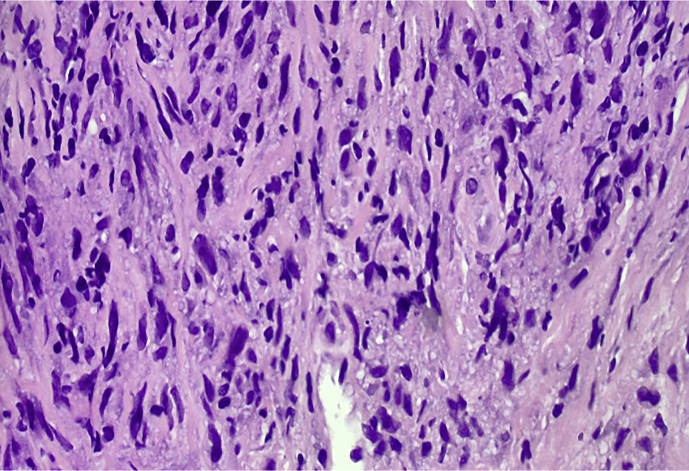
Case report: We present a rare case of PMBCL in a 39-year-old male with a bulky mediastinal mass that resulted in superior vena cava thrombosis and cardiac tamponade. Diagnostic discordance between histopathological and molecular data led to a delay in interception of this entity. Histopathology findings were suggestive of spindle-cell neoplasm. Contrastingly, next-generation sequencing (NGS) and immunohistochemistry (IHC) yielded a molecular diagnosis of PMBCL. IHC staining revealed that the atypical cells were positive for CD20, PAX5, CD79a, CD30, CD23, MUM1, and weakly positive for MAL (myelin and lymphocyte) protein. NGS showed increased expression of TNFRSF8 and CD274 genes, which encode CD30 and PDL1 proteins, respectively. The patient was successfully treated with the R-Hyper-CVAD protocol without consolidative radiotherapy.
Conclusion: Diagnosing PMBCL can be challenging because it lacks pathognomonic features and shares characteristics with other lymphomas. Molecular testing is of paramount importance in this context owing to its distinctive immunophenotype.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


