Erica N Presnell, Andrea M Bond, Jessica Hernandez
{"title":"经皮介入治疗(EVADE PCI)后急性和早期P2Y12抑制剂降级的评价","authors":"Erica N Presnell, Andrea M Bond, Jessica Hernandez","doi":"10.17161/kjm.vol18.22921","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Aspirin and an oral P2Y12 inhibitor are recommended for one year after percutaneous coronary intervention (PCI) in patients with acute coronary syndromes. While ticagrelor or prasugrel, more potent P2Y12 inhibitors, are preferred over clopidogrel, de-escalation often is based on provider judgment. This study compared cardiovascular outcomes and bleeding risks between patients who remained on ticagrelor or prasugrel (unchanged group) and those de-escalated to clopidogrel within 30 days of PCI.</p><p><strong>Methods: </strong>The authors analyzed data from patients admitted between June 2014 and December 2022 for acute coronary syndromes requiring PCI who received an oral P2Y12 inhibitor within 72 hours of admission. The primary outcome was a composite of all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding at one year. Secondary outcomes included the individual components of the composite outcome. Statistical analyses included chi-square tests, Student's t-tests, or non-parametric equivalents, as appropriate.</p><p><strong>Results: </strong>A total of 210 patients met the inclusion criteria, with 149 remaining on unchanged P2Y12 therapy and 61 undergoing de-escalation. There was no statistically significant difference in the composite outcome between the unchanged and de-escalated groups (n [%]: 25 [17] vs. 6 [10]; χ<sup>2</sup> [1, N = 210] = 1.658, p = 0.198). Additionally, secondary outcomes, including all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding, did not differ significantly between groups.</p><p><strong>Conclusions: </strong>A composite outcome of all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding at one year was similar between patients who continued ticagrelor or prasugrel and those de-escalated to clopidogrel within 30 days of PCI. Larger studies are needed to confirm these findings and assess the optimal timing for therapy adjustments.</p>","PeriodicalId":94121,"journal":{"name":"Kansas journal of medicine","volume":"18 2","pages":"31-34"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12135783/pdf/","citationCount":"0","resultStr":"{\"title\":\"EValuation of Acute and Early Phase P2Y12 Inhibitor DE-escalation After PerCutaneous Intervention (EVADE PCI).\",\"authors\":\"Erica N Presnell, Andrea M Bond, Jessica Hernandez\",\"doi\":\"10.17161/kjm.vol18.22921\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Aspirin and an oral P2Y12 inhibitor are recommended for one year after percutaneous coronary intervention (PCI) in patients with acute coronary syndromes. While ticagrelor or prasugrel, more potent P2Y12 inhibitors, are preferred over clopidogrel, de-escalation often is based on provider judgment. This study compared cardiovascular outcomes and bleeding risks between patients who remained on ticagrelor or prasugrel (unchanged group) and those de-escalated to clopidogrel within 30 days of PCI.</p><p><strong>Methods: </strong>The authors analyzed data from patients admitted between June 2014 and December 2022 for acute coronary syndromes requiring PCI who received an oral P2Y12 inhibitor within 72 hours of admission. The primary outcome was a composite of all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding at one year. Secondary outcomes included the individual components of the composite outcome. Statistical analyses included chi-square tests, Student's t-tests, or non-parametric equivalents, as appropriate.</p><p><strong>Results: </strong>A total of 210 patients met the inclusion criteria, with 149 remaining on unchanged P2Y12 therapy and 61 undergoing de-escalation. There was no statistically significant difference in the composite outcome between the unchanged and de-escalated groups (n [%]: 25 [17] vs. 6 [10]; χ<sup>2</sup> [1, N = 210] = 1.658, p = 0.198). Additionally, secondary outcomes, including all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding, did not differ significantly between groups.</p><p><strong>Conclusions: </strong>A composite outcome of all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding at one year was similar between patients who continued ticagrelor or prasugrel and those de-escalated to clopidogrel within 30 days of PCI. Larger studies are needed to confirm these findings and assess the optimal timing for therapy adjustments.</p>\",\"PeriodicalId\":94121,\"journal\":{\"name\":\"Kansas journal of medicine\",\"volume\":\"18 2\",\"pages\":\"31-34\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12135783/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Kansas journal of medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.17161/kjm.vol18.22921\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kansas journal of medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17161/kjm.vol18.22921","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
急性冠脉综合征患者经皮冠状动脉介入治疗(PCI)后,推荐服用阿司匹林和口服P2Y12抑制剂一年。与氯吡格雷相比,替格瑞或普拉格雷是更有效的P2Y12抑制剂,但降级通常是基于提供者的判断。该研究比较了PCI术后30天内继续使用替格瑞或普拉格雷(不变组)和减少使用氯吡格雷的患者的心血管结局和出血风险。方法:作者分析了2014年6月至2022年12月入院的急性冠状动脉综合征患者的数据,这些患者在入院72小时内接受了口服P2Y12抑制剂。主要结局是一年内全因死亡率、紧急血运重建、支架血栓形成、中风和大出血的综合结果。次要结局包括复合结局的各个组成部分。统计分析包括卡方检验、学生t检验或适当的非参数等效检验。结果:共有210名患者符合纳入标准,其中149名患者继续接受不变的P2Y12治疗,61名患者接受降压治疗。不变组和降级组的综合结局无统计学差异(n [%]: 25 [17] vs. 6 [10];χ2 [1, N = 210] = 1.658, p = 0.198)。此外,次要结局,包括全因死亡率、紧急血运重建术、支架血栓形成、中风和大出血,组间无显著差异。结论:在PCI术后30天内继续使用替格瑞或普拉格雷的患者与逐渐停用氯吡格雷的患者之间,一年内全因死亡率、紧急血运重建、支架血栓形成、卒中和大出血的综合结果相似。需要更大规模的研究来证实这些发现,并评估调整治疗的最佳时机。
EValuation of Acute and Early Phase P2Y12 Inhibitor DE-escalation After PerCutaneous Intervention (EVADE PCI).
Introduction: Aspirin and an oral P2Y12 inhibitor are recommended for one year after percutaneous coronary intervention (PCI) in patients with acute coronary syndromes. While ticagrelor or prasugrel, more potent P2Y12 inhibitors, are preferred over clopidogrel, de-escalation often is based on provider judgment. This study compared cardiovascular outcomes and bleeding risks between patients who remained on ticagrelor or prasugrel (unchanged group) and those de-escalated to clopidogrel within 30 days of PCI.
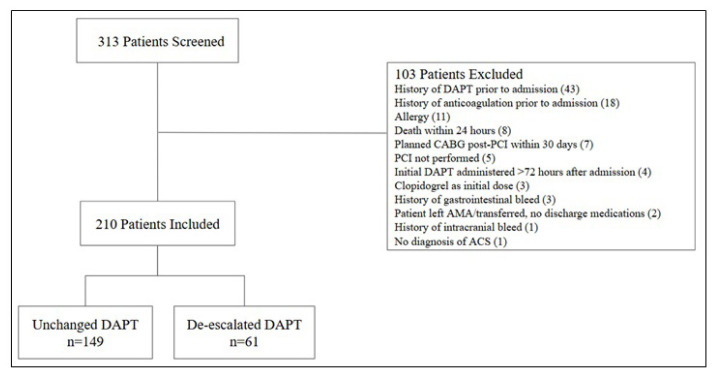
Methods: The authors analyzed data from patients admitted between June 2014 and December 2022 for acute coronary syndromes requiring PCI who received an oral P2Y12 inhibitor within 72 hours of admission. The primary outcome was a composite of all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding at one year. Secondary outcomes included the individual components of the composite outcome. Statistical analyses included chi-square tests, Student's t-tests, or non-parametric equivalents, as appropriate.
Results: A total of 210 patients met the inclusion criteria, with 149 remaining on unchanged P2Y12 therapy and 61 undergoing de-escalation. There was no statistically significant difference in the composite outcome between the unchanged and de-escalated groups (n [%]: 25 [17] vs. 6 [10]; χ2 [1, N = 210] = 1.658, p = 0.198). Additionally, secondary outcomes, including all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding, did not differ significantly between groups.
Conclusions: A composite outcome of all-cause mortality, urgent revascularization, stent thrombosis, stroke, and major bleeding at one year was similar between patients who continued ticagrelor or prasugrel and those de-escalated to clopidogrel within 30 days of PCI. Larger studies are needed to confirm these findings and assess the optimal timing for therapy adjustments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


