Otis C van Varsseveld, Floris V Raasveld, Wen-Chih Liu, Justin McCarty, Caroline A Hundepool, J Michiel Zuidam, Ian L Valerio, Kyle R Eberlin
{"title":"膝关节置换术后周围神经症状的外科治疗。","authors":"Otis C van Varsseveld, Floris V Raasveld, Wen-Chih Liu, Justin McCarty, Caroline A Hundepool, J Michiel Zuidam, Ian L Valerio, Kyle R Eberlin","doi":"10.1186/s42836-025-00315-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neuropathic pain, weakness, and/or numbness can complicate partial or total knee arthroplasty (KA). This study evaluates peripheral nerve surgery following KA and proposes a treatment algorithm.</p><p><strong>Methods: </strong>Patients who underwent peripheral nerve surgery for neuropathic symptoms (neuropathic pain and/or motor dysfunction) following KA between 2012-2024 (≥ 3-month follow-up) were included. Demographics, comorbidities, and type of treatment were collected, and a cross-sectional survey assessed satisfaction (Patient Global Impression of Change, PGIC) and quality of life (EuroQol-5-Dimension-5-Level, EQ-5D-5L).</p><p><strong>Results: </strong>Twenty-seven lower extremities treated in 26 patients with a median age of 67.0 years (IQR: 58.0-71.8) were included. Surgical indications included neuropathic pain (n = 24/27, 88.9%), foot drop (n = 1/27, 3.7%), or both (n = 2/27, 7.4%). Median time between KA and nerve surgery was 29.5 months (IQR: 12.5-71.0). Procedures included saphenous or infrapatellar branch neurectomy with active management of the nerve ending (targeted muscle reinnervation (TMR) or regenerative peripheral nerve interface (RPNI)) (48.1%, n = 13), nerve decompression (40.7%, n = 11), or a combination of the two (11.1%, n = 3). Twenty-one patients (80.8%, 22 extremities) completed the survey with a median follow-up of 1.9 years (IQR: 1.1-4.2). Improvement (PGIC) was reported in 21 extremities (95.5%), the mean EQ-5D-5L index was 0.854 (± 0.102) (US general population: 0.851 (± 0.205)).</p><p><strong>Conclusion: </strong>Peripheral nerve surgery is beneficial for patients with neuropathic pain, numbness, and/or weakness following KA. We recommend common peroneal nerve decompression for lateral knee pain and/or foot drop, active saphenous nerve management with TMR or RPNI for medial knee pain, or a combination of the two based on the clinical scenario. These findings may aid in the decision-making process for patients with neuropathic pain following KA and warrant further validation in larger, prospective studies.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":"7 1","pages":"27"},"PeriodicalIF":4.3000,"publicationDate":"2025-06-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12142898/pdf/","citationCount":"0","resultStr":"{\"title\":\"Surgical management of peripheral nerve symptoms following knee arthroplasty.\",\"authors\":\"Otis C van Varsseveld, Floris V Raasveld, Wen-Chih Liu, Justin McCarty, Caroline A Hundepool, J Michiel Zuidam, Ian L Valerio, Kyle R Eberlin\",\"doi\":\"10.1186/s42836-025-00315-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Neuropathic pain, weakness, and/or numbness can complicate partial or total knee arthroplasty (KA). This study evaluates peripheral nerve surgery following KA and proposes a treatment algorithm.</p><p><strong>Methods: </strong>Patients who underwent peripheral nerve surgery for neuropathic symptoms (neuropathic pain and/or motor dysfunction) following KA between 2012-2024 (≥ 3-month follow-up) were included. Demographics, comorbidities, and type of treatment were collected, and a cross-sectional survey assessed satisfaction (Patient Global Impression of Change, PGIC) and quality of life (EuroQol-5-Dimension-5-Level, EQ-5D-5L).</p><p><strong>Results: </strong>Twenty-seven lower extremities treated in 26 patients with a median age of 67.0 years (IQR: 58.0-71.8) were included. Surgical indications included neuropathic pain (n = 24/27, 88.9%), foot drop (n = 1/27, 3.7%), or both (n = 2/27, 7.4%). Median time between KA and nerve surgery was 29.5 months (IQR: 12.5-71.0). Procedures included saphenous or infrapatellar branch neurectomy with active management of the nerve ending (targeted muscle reinnervation (TMR) or regenerative peripheral nerve interface (RPNI)) (48.1%, n = 13), nerve decompression (40.7%, n = 11), or a combination of the two (11.1%, n = 3). Twenty-one patients (80.8%, 22 extremities) completed the survey with a median follow-up of 1.9 years (IQR: 1.1-4.2). Improvement (PGIC) was reported in 21 extremities (95.5%), the mean EQ-5D-5L index was 0.854 (± 0.102) (US general population: 0.851 (± 0.205)).</p><p><strong>Conclusion: </strong>Peripheral nerve surgery is beneficial for patients with neuropathic pain, numbness, and/or weakness following KA. We recommend common peroneal nerve decompression for lateral knee pain and/or foot drop, active saphenous nerve management with TMR or RPNI for medial knee pain, or a combination of the two based on the clinical scenario. These findings may aid in the decision-making process for patients with neuropathic pain following KA and warrant further validation in larger, prospective studies.</p>\",\"PeriodicalId\":52831,\"journal\":{\"name\":\"Arthroplasty\",\"volume\":\"7 1\",\"pages\":\"27\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2025-06-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12142898/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthroplasty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s42836-025-00315-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-025-00315-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Surgical management of peripheral nerve symptoms following knee arthroplasty.
Background: Neuropathic pain, weakness, and/or numbness can complicate partial or total knee arthroplasty (KA). This study evaluates peripheral nerve surgery following KA and proposes a treatment algorithm.
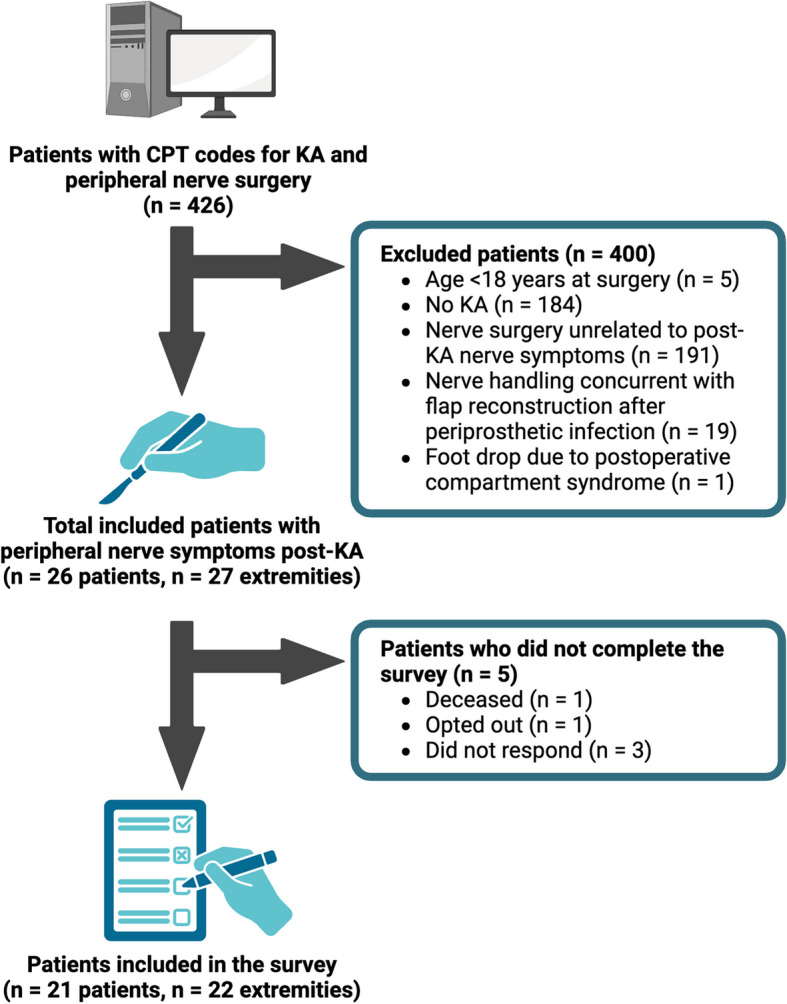
Methods: Patients who underwent peripheral nerve surgery for neuropathic symptoms (neuropathic pain and/or motor dysfunction) following KA between 2012-2024 (≥ 3-month follow-up) were included. Demographics, comorbidities, and type of treatment were collected, and a cross-sectional survey assessed satisfaction (Patient Global Impression of Change, PGIC) and quality of life (EuroQol-5-Dimension-5-Level, EQ-5D-5L).
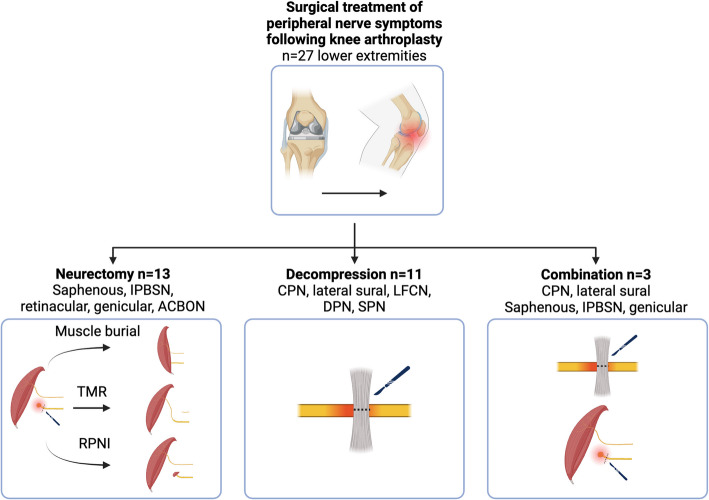
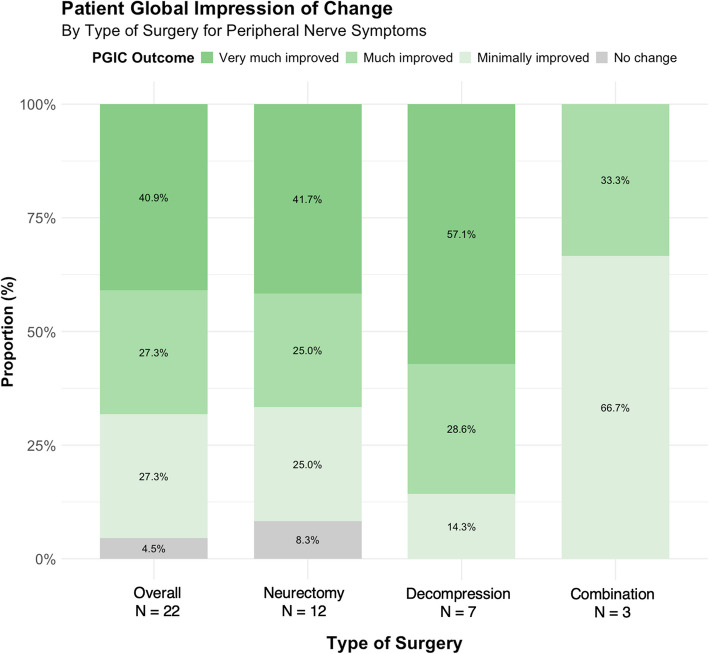
Results: Twenty-seven lower extremities treated in 26 patients with a median age of 67.0 years (IQR: 58.0-71.8) were included. Surgical indications included neuropathic pain (n = 24/27, 88.9%), foot drop (n = 1/27, 3.7%), or both (n = 2/27, 7.4%). Median time between KA and nerve surgery was 29.5 months (IQR: 12.5-71.0). Procedures included saphenous or infrapatellar branch neurectomy with active management of the nerve ending (targeted muscle reinnervation (TMR) or regenerative peripheral nerve interface (RPNI)) (48.1%, n = 13), nerve decompression (40.7%, n = 11), or a combination of the two (11.1%, n = 3). Twenty-one patients (80.8%, 22 extremities) completed the survey with a median follow-up of 1.9 years (IQR: 1.1-4.2). Improvement (PGIC) was reported in 21 extremities (95.5%), the mean EQ-5D-5L index was 0.854 (± 0.102) (US general population: 0.851 (± 0.205)).
Conclusion: Peripheral nerve surgery is beneficial for patients with neuropathic pain, numbness, and/or weakness following KA. We recommend common peroneal nerve decompression for lateral knee pain and/or foot drop, active saphenous nerve management with TMR or RPNI for medial knee pain, or a combination of the two based on the clinical scenario. These findings may aid in the decision-making process for patients with neuropathic pain following KA and warrant further validation in larger, prospective studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


