Ekta Jain, Jorge A Diaz, Mustafa Goksel, Arnab Basu, Cristina Magi-Galluzzi
{"title":"免疫检查点抑制剂治疗转移性肾癌:肿瘤反应和细胞减少性肾切除术后的免疫相关肾血管炎。","authors":"Ekta Jain, Jorge A Diaz, Mustafa Goksel, Arnab Basu, Cristina Magi-Galluzzi","doi":"10.32074/1591-951X-N998","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Therapeutic landscape of metastatic renal cell carcinoma (mRCC) has transformed over the last 2 decades, particularly with the advent of immune checkpoint inhibitors (ICI). While ICI offer therapeutic benefits, they can also provoke immune-related adverse events (iRAEs). Vasculitis as a clinical iRAE from ICI is rare in association with RCC treatment.</p><p><strong>Methods: </strong>This study included patients treated at our institution with ICI for mRCC (2019-2024). We collected clinicopathologic data and type and duration of immunotherapy. Histologic sections of tumors were re-reviewed by two pathologists to determine pathologic response and features of ICI-related renal injuries.</p><p><strong>Results: </strong>We identified 8 patients (median age 61.5 years) of which six (75%) presented with metastases at multiple sites, while two had recurrent oligometastatic disease post-partial nephrectomy. All patients were treated with ICI for a duration ranging from 6 to 20 months; 7 patients received combination therapy (CT) [iplimumab & nivolumab (n = 3), pembrolizumab & lenvatinib (n = 2), nivolumab & carbozantinib (n = 1), pembrolizumab & axitinib (n = 1)], while one received monotherapy (MT) (pembrolizumab). Patients were poor surgical candidates at diagnosis (25% Stage 3, 75% stage 4). Six (75%) patients had clear cell RCC (CCRCC), 2 patients had RCC with papillary and eosinophilic features. Tumor necrosis was noted in 75% of cases. Partial tumor response occurred in 7 (87.5%) patients, with 3 (37.5%) achieving tumor downstaging. One patient showed stable primary disease despite resolution of metastatic burden and none of the patients achieved complete response. Three patients (37.5%) had histopathological confirmed renal iRAEs. Two (25%) patients displayed vascular lymphocytic infiltrates, consistent with medium vessels vasculitis; they received CT for 6 months. One patient, who received CT for 20 months, showed a non-necrotizing granuloma.</p><p><strong>Conclusions: </strong>This study highlights the potential of ICIs for tumor downstaging and disease control in mRCC, though further investigation is warranted to optimize management of iRAEs and long-term outcomes. ICI-associated renal vasculitis is likely underrecognized and underreported highlighting the need for thorough pathological evaluation of non-neoplastic renal tissue in patients receiving ICI.</p>","PeriodicalId":45893,"journal":{"name":"PATHOLOGICA","volume":" ","pages":"249-257"},"PeriodicalIF":2.9000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12236139/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immune checkpoint inhibitor therapy in metastatic renal cell carcinoma: tumour response and immune-related renal vasculitis following cytoreductive nephrectomy.\",\"authors\":\"Ekta Jain, Jorge A Diaz, Mustafa Goksel, Arnab Basu, Cristina Magi-Galluzzi\",\"doi\":\"10.32074/1591-951X-N998\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Therapeutic landscape of metastatic renal cell carcinoma (mRCC) has transformed over the last 2 decades, particularly with the advent of immune checkpoint inhibitors (ICI). While ICI offer therapeutic benefits, they can also provoke immune-related adverse events (iRAEs). Vasculitis as a clinical iRAE from ICI is rare in association with RCC treatment.</p><p><strong>Methods: </strong>This study included patients treated at our institution with ICI for mRCC (2019-2024). We collected clinicopathologic data and type and duration of immunotherapy. Histologic sections of tumors were re-reviewed by two pathologists to determine pathologic response and features of ICI-related renal injuries.</p><p><strong>Results: </strong>We identified 8 patients (median age 61.5 years) of which six (75%) presented with metastases at multiple sites, while two had recurrent oligometastatic disease post-partial nephrectomy. All patients were treated with ICI for a duration ranging from 6 to 20 months; 7 patients received combination therapy (CT) [iplimumab & nivolumab (n = 3), pembrolizumab & lenvatinib (n = 2), nivolumab & carbozantinib (n = 1), pembrolizumab & axitinib (n = 1)], while one received monotherapy (MT) (pembrolizumab). Patients were poor surgical candidates at diagnosis (25% Stage 3, 75% stage 4). Six (75%) patients had clear cell RCC (CCRCC), 2 patients had RCC with papillary and eosinophilic features. Tumor necrosis was noted in 75% of cases. Partial tumor response occurred in 7 (87.5%) patients, with 3 (37.5%) achieving tumor downstaging. One patient showed stable primary disease despite resolution of metastatic burden and none of the patients achieved complete response. Three patients (37.5%) had histopathological confirmed renal iRAEs. Two (25%) patients displayed vascular lymphocytic infiltrates, consistent with medium vessels vasculitis; they received CT for 6 months. One patient, who received CT for 20 months, showed a non-necrotizing granuloma.</p><p><strong>Conclusions: </strong>This study highlights the potential of ICIs for tumor downstaging and disease control in mRCC, though further investigation is warranted to optimize management of iRAEs and long-term outcomes. ICI-associated renal vasculitis is likely underrecognized and underreported highlighting the need for thorough pathological evaluation of non-neoplastic renal tissue in patients receiving ICI.</p>\",\"PeriodicalId\":45893,\"journal\":{\"name\":\"PATHOLOGICA\",\"volume\":\" \",\"pages\":\"249-257\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12236139/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PATHOLOGICA\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.32074/1591-951X-N998\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PATHOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PATHOLOGICA","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.32074/1591-951X-N998","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PATHOLOGY","Score":null,"Total":0}
Immune checkpoint inhibitor therapy in metastatic renal cell carcinoma: tumour response and immune-related renal vasculitis following cytoreductive nephrectomy.
Objective: Therapeutic landscape of metastatic renal cell carcinoma (mRCC) has transformed over the last 2 decades, particularly with the advent of immune checkpoint inhibitors (ICI). While ICI offer therapeutic benefits, they can also provoke immune-related adverse events (iRAEs). Vasculitis as a clinical iRAE from ICI is rare in association with RCC treatment.
Methods: This study included patients treated at our institution with ICI for mRCC (2019-2024). We collected clinicopathologic data and type and duration of immunotherapy. Histologic sections of tumors were re-reviewed by two pathologists to determine pathologic response and features of ICI-related renal injuries.
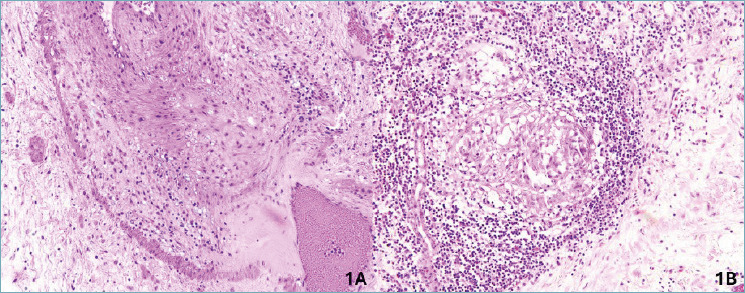
Results: We identified 8 patients (median age 61.5 years) of which six (75%) presented with metastases at multiple sites, while two had recurrent oligometastatic disease post-partial nephrectomy. All patients were treated with ICI for a duration ranging from 6 to 20 months; 7 patients received combination therapy (CT) [iplimumab & nivolumab (n = 3), pembrolizumab & lenvatinib (n = 2), nivolumab & carbozantinib (n = 1), pembrolizumab & axitinib (n = 1)], while one received monotherapy (MT) (pembrolizumab). Patients were poor surgical candidates at diagnosis (25% Stage 3, 75% stage 4). Six (75%) patients had clear cell RCC (CCRCC), 2 patients had RCC with papillary and eosinophilic features. Tumor necrosis was noted in 75% of cases. Partial tumor response occurred in 7 (87.5%) patients, with 3 (37.5%) achieving tumor downstaging. One patient showed stable primary disease despite resolution of metastatic burden and none of the patients achieved complete response. Three patients (37.5%) had histopathological confirmed renal iRAEs. Two (25%) patients displayed vascular lymphocytic infiltrates, consistent with medium vessels vasculitis; they received CT for 6 months. One patient, who received CT for 20 months, showed a non-necrotizing granuloma.
Conclusions: This study highlights the potential of ICIs for tumor downstaging and disease control in mRCC, though further investigation is warranted to optimize management of iRAEs and long-term outcomes. ICI-associated renal vasculitis is likely underrecognized and underreported highlighting the need for thorough pathological evaluation of non-neoplastic renal tissue in patients receiving ICI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


