{"title":"万古霉素监测治疗成人囊性纤维化患者急性肺加重。","authors":"Darrell Smith, James Sanders, Marguerite Monogue","doi":"10.1155/pm/5683225","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Therapeutic drug monitoring (TDM) for vancomycin (VAN) in adult people with cystic fibrosis (pwCF) historically has utilized trough concentrations. Recent VAN TDM guidelines recommend area under the curve (AUC) monitoring to reduce the risk of acute kidney injury (AKI), despite limited evidence to support this practice in adult pwCF. <b>Methods:</b> This single-center, retrospective, observational cohort study included 143 adult pwCF admitted from July 1, 2017, to July 1, 2022, with an acute pulmonary exacerbation that received VAN for at least 72 h with available VAN plasma concentrations for TDM for AUC (<i>n</i> = 39) or trough monitoring (<i>n</i> = 104). Eligible patients with multiple hospital admissions during the study period were incorporated as separate encounters. The primary outcome was the incidence of AKI. <b>Results:</b> Receipt of concurrent nephrotoxins was more common in the AUC cohort than in the trough cohort (97% vs. 81%, <i>p</i> = 0.01), but the rate of AKI was similar (7.7% vs. 10.6%, <i>p</i> = 0.76). AUC monitoring was associated with earlier achievement of TDM goal (median 0 days (IQR 0-2) vs. 2 days (IQR 0-4), <i>p</i> < 0.01), lower total daily doses (34.8 mg/kg/day (IQR 27.6-49) vs. 57.5 mg/kg/day (IQR 43.9-68.6), <i>p</i> < 0.01), and fewer regimen changes (median 1 change (IQR 0-2) vs. 2 changes (IQR 1-3), <i>p</i> < 0.01). In patients with MRSA, pulmonary function recovery, readmission, and mortality were similar. <b>Conclusion:</b> In adult pwCF, the incidence of AKI was similar between AUC and trough monitoring cohorts; however, AUC monitoring achieved therapeutic targets sooner with fewer regimen modifications without significantly increasing the number of concentrations compared to trough monitoring.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2025 ","pages":"5683225"},"PeriodicalIF":2.1000,"publicationDate":"2025-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136855/pdf/","citationCount":"0","resultStr":"{\"title\":\"Vancomycin Monitoring for Treatment of Acute Pulmonary Exacerbations of Adult Cystic Fibrosis Patients.\",\"authors\":\"Darrell Smith, James Sanders, Marguerite Monogue\",\"doi\":\"10.1155/pm/5683225\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Therapeutic drug monitoring (TDM) for vancomycin (VAN) in adult people with cystic fibrosis (pwCF) historically has utilized trough concentrations. Recent VAN TDM guidelines recommend area under the curve (AUC) monitoring to reduce the risk of acute kidney injury (AKI), despite limited evidence to support this practice in adult pwCF. <b>Methods:</b> This single-center, retrospective, observational cohort study included 143 adult pwCF admitted from July 1, 2017, to July 1, 2022, with an acute pulmonary exacerbation that received VAN for at least 72 h with available VAN plasma concentrations for TDM for AUC (<i>n</i> = 39) or trough monitoring (<i>n</i> = 104). Eligible patients with multiple hospital admissions during the study period were incorporated as separate encounters. The primary outcome was the incidence of AKI. <b>Results:</b> Receipt of concurrent nephrotoxins was more common in the AUC cohort than in the trough cohort (97% vs. 81%, <i>p</i> = 0.01), but the rate of AKI was similar (7.7% vs. 10.6%, <i>p</i> = 0.76). AUC monitoring was associated with earlier achievement of TDM goal (median 0 days (IQR 0-2) vs. 2 days (IQR 0-4), <i>p</i> < 0.01), lower total daily doses (34.8 mg/kg/day (IQR 27.6-49) vs. 57.5 mg/kg/day (IQR 43.9-68.6), <i>p</i> < 0.01), and fewer regimen changes (median 1 change (IQR 0-2) vs. 2 changes (IQR 1-3), <i>p</i> < 0.01). In patients with MRSA, pulmonary function recovery, readmission, and mortality were similar. <b>Conclusion:</b> In adult pwCF, the incidence of AKI was similar between AUC and trough monitoring cohorts; however, AUC monitoring achieved therapeutic targets sooner with fewer regimen modifications without significantly increasing the number of concentrations compared to trough monitoring.</p>\",\"PeriodicalId\":46434,\"journal\":{\"name\":\"Pulmonary Medicine\",\"volume\":\"2025 \",\"pages\":\"5683225\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-05-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12136855/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/pm/5683225\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/pm/5683225","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
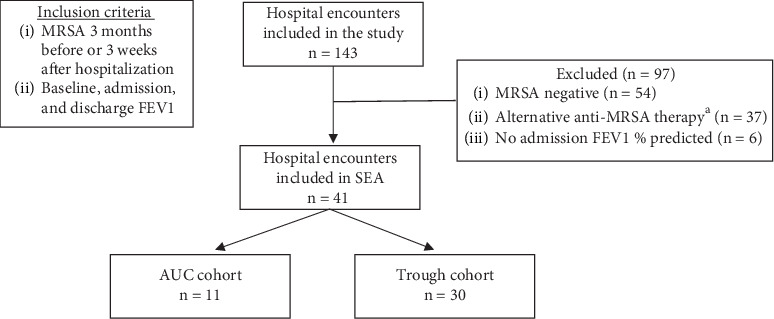
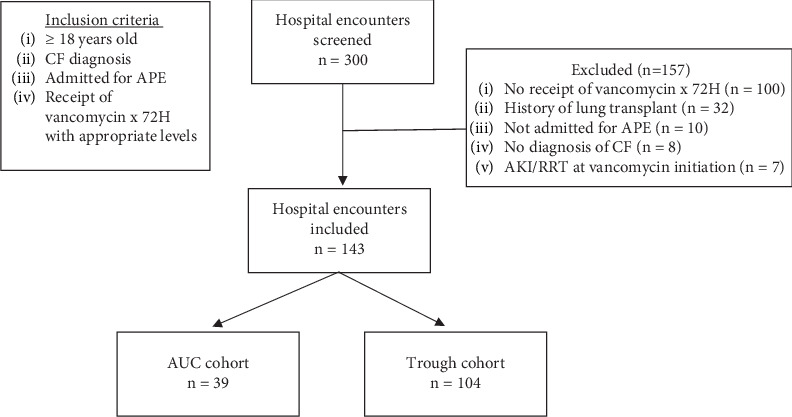
背景:成人囊性纤维化(pwCF)患者万古霉素(VAN)的治疗药物监测(TDM)历来使用谷浓度。最近的VAN TDM指南推荐曲线下面积(AUC)监测来降低急性肾损伤(AKI)的风险,尽管在成人pwCF中支持这种做法的证据有限。方法:这项单中心、回顾性、观察性队列研究纳入了2017年7月1日至2022年7月1日收治的143例成年pwCF患者,这些患者急性肺恶化接受VAN治疗至少72小时,并伴有AUC TDM可用VAN血浆浓度(n = 39)或槽监测(n = 104)。在研究期间多次住院的符合条件的患者被纳入单独的接触。主要终点是AKI的发生率。结果:AUC组并发肾毒素比低谷组更常见(97%对81%,p = 0.01),但AKI发生率相似(7.7%对10.6%,p = 0.76)。AUC监测与TDM目标的早期实现(中位0天(IQR 0-2) vs. 2天(IQR 0-4), p < 0.01),较低的总日剂量(34.8 mg/kg/天(IQR 27.6-49) vs. 57.5 mg/kg/天(IQR 43.9-68.6), p < 0.01),较少的方案变化(中位1次变化(IQR 0-2) vs. 2次变化(IQR 1-3), p < 0.01)相关。在MRSA患者中,肺功能恢复、再入院和死亡率相似。结论:在成人pwCF中,AUC组和低谷监测组的AKI发生率相似;然而,与低谷监测相比,AUC监测更快地实现了治疗目标,较少的方案修改,而没有显著增加浓度的数量。
Vancomycin Monitoring for Treatment of Acute Pulmonary Exacerbations of Adult Cystic Fibrosis Patients.
Background: Therapeutic drug monitoring (TDM) for vancomycin (VAN) in adult people with cystic fibrosis (pwCF) historically has utilized trough concentrations. Recent VAN TDM guidelines recommend area under the curve (AUC) monitoring to reduce the risk of acute kidney injury (AKI), despite limited evidence to support this practice in adult pwCF. Methods: This single-center, retrospective, observational cohort study included 143 adult pwCF admitted from July 1, 2017, to July 1, 2022, with an acute pulmonary exacerbation that received VAN for at least 72 h with available VAN plasma concentrations for TDM for AUC (n = 39) or trough monitoring (n = 104). Eligible patients with multiple hospital admissions during the study period were incorporated as separate encounters. The primary outcome was the incidence of AKI. Results: Receipt of concurrent nephrotoxins was more common in the AUC cohort than in the trough cohort (97% vs. 81%, p = 0.01), but the rate of AKI was similar (7.7% vs. 10.6%, p = 0.76). AUC monitoring was associated with earlier achievement of TDM goal (median 0 days (IQR 0-2) vs. 2 days (IQR 0-4), p < 0.01), lower total daily doses (34.8 mg/kg/day (IQR 27.6-49) vs. 57.5 mg/kg/day (IQR 43.9-68.6), p < 0.01), and fewer regimen changes (median 1 change (IQR 0-2) vs. 2 changes (IQR 1-3), p < 0.01). In patients with MRSA, pulmonary function recovery, readmission, and mortality were similar. Conclusion: In adult pwCF, the incidence of AKI was similar between AUC and trough monitoring cohorts; however, AUC monitoring achieved therapeutic targets sooner with fewer regimen modifications without significantly increasing the number of concentrations compared to trough monitoring.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


