Alexander Marschall, Freddy Delgado Calva, Inés Gómez Sánchez, Elena Basabe Velasco, Manuel Tapia Martinez, David Martí Sánchez
{"title":"总体纵向应变与左心室射血分数对无症状稳定型心力衰竭患者短期临床进展的预测","authors":"Alexander Marschall, Freddy Delgado Calva, Inés Gómez Sánchez, Elena Basabe Velasco, Manuel Tapia Martinez, David Martí Sánchez","doi":"10.4103/jcecho.jcecho_28_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Left ventricular global longitudinal strain (LV GLS) has shown to allow for risk stratification in heart failure (HF) patients with greater accuracy than LV ejection fraction (LVEF). However, previous studies included only few patients in New York Heart Association (NYHA) functional class I and rarely assessed clinical stability. The aim of this study was to determine the predictive value of LV GLS, as compared to LVEF, for short-term disease progression in asymptomatic stable HF patients.</p><p><strong>Methods: </strong>This is a retrospective study including consecutive HF patients with LVEF <50%, in NYHA I, with no history of decompensation within the previous 6 months. The primary endpoint was the composite of cardiovascular death, hospitalization, and need for intensification of HF treatment within a 12-month follow-up period.</p><p><strong>Results: </strong>Out of 153 patients, 17.8% showed disease progression. Receiver operating characteristic curves identified GLS as the most accurate predictor for clinical progression (area under the curve [AUC]: 0.883 (95% confidence interval [CI]: 0.811-0.954), cutoff: -9.0%, sensitivity: 88.5%, and specificity: 88.5%). LVEF performed less precisely (AUC: 0.654 [95% CI: 0.527-0.782], cutoff: 42%, sensitivity: 70.4%, and specificity: 54%). Depressed GLS was a strong and significant predictor for disease progression (hazard ratio [HR]: 16.7 (95% CI: 6.2-35.1), <i>P</i> < 0.001). Reduced LVEF showed to be a less reliable predictor (HR: 2.4 [95% CI: 1.1-5.2]).</p><p><strong>Conclusions: </strong>GLS reliably predicts clinical progression in asymptomatic stable HF patients, with greater accuracy than LVEF. Its implementation in the risk stratification of these patients could help to identify those patients who are at greatest risk and may benefit from an intensification of their follow up and/or HF treatment.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"35 1","pages":"32-36"},"PeriodicalIF":1.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12129269/pdf/","citationCount":"0","resultStr":"{\"title\":\"Global Longitudinal Strain versus Left Ventricular Ejection Fraction for the Prediction of Short-term Clinical Progression in Asymptomatic Stable Heart Failure Patients.\",\"authors\":\"Alexander Marschall, Freddy Delgado Calva, Inés Gómez Sánchez, Elena Basabe Velasco, Manuel Tapia Martinez, David Martí Sánchez\",\"doi\":\"10.4103/jcecho.jcecho_28_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Left ventricular global longitudinal strain (LV GLS) has shown to allow for risk stratification in heart failure (HF) patients with greater accuracy than LV ejection fraction (LVEF). However, previous studies included only few patients in New York Heart Association (NYHA) functional class I and rarely assessed clinical stability. The aim of this study was to determine the predictive value of LV GLS, as compared to LVEF, for short-term disease progression in asymptomatic stable HF patients.</p><p><strong>Methods: </strong>This is a retrospective study including consecutive HF patients with LVEF <50%, in NYHA I, with no history of decompensation within the previous 6 months. The primary endpoint was the composite of cardiovascular death, hospitalization, and need for intensification of HF treatment within a 12-month follow-up period.</p><p><strong>Results: </strong>Out of 153 patients, 17.8% showed disease progression. Receiver operating characteristic curves identified GLS as the most accurate predictor for clinical progression (area under the curve [AUC]: 0.883 (95% confidence interval [CI]: 0.811-0.954), cutoff: -9.0%, sensitivity: 88.5%, and specificity: 88.5%). LVEF performed less precisely (AUC: 0.654 [95% CI: 0.527-0.782], cutoff: 42%, sensitivity: 70.4%, and specificity: 54%). Depressed GLS was a strong and significant predictor for disease progression (hazard ratio [HR]: 16.7 (95% CI: 6.2-35.1), <i>P</i> < 0.001). Reduced LVEF showed to be a less reliable predictor (HR: 2.4 [95% CI: 1.1-5.2]).</p><p><strong>Conclusions: </strong>GLS reliably predicts clinical progression in asymptomatic stable HF patients, with greater accuracy than LVEF. Its implementation in the risk stratification of these patients could help to identify those patients who are at greatest risk and may benefit from an intensification of their follow up and/or HF treatment.</p>\",\"PeriodicalId\":15191,\"journal\":{\"name\":\"Journal of Cardiovascular Echography\",\"volume\":\"35 1\",\"pages\":\"32-36\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12129269/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Echography\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcecho.jcecho_28_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_28_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Global Longitudinal Strain versus Left Ventricular Ejection Fraction for the Prediction of Short-term Clinical Progression in Asymptomatic Stable Heart Failure Patients.
Background: Left ventricular global longitudinal strain (LV GLS) has shown to allow for risk stratification in heart failure (HF) patients with greater accuracy than LV ejection fraction (LVEF). However, previous studies included only few patients in New York Heart Association (NYHA) functional class I and rarely assessed clinical stability. The aim of this study was to determine the predictive value of LV GLS, as compared to LVEF, for short-term disease progression in asymptomatic stable HF patients.
Methods: This is a retrospective study including consecutive HF patients with LVEF <50%, in NYHA I, with no history of decompensation within the previous 6 months. The primary endpoint was the composite of cardiovascular death, hospitalization, and need for intensification of HF treatment within a 12-month follow-up period.
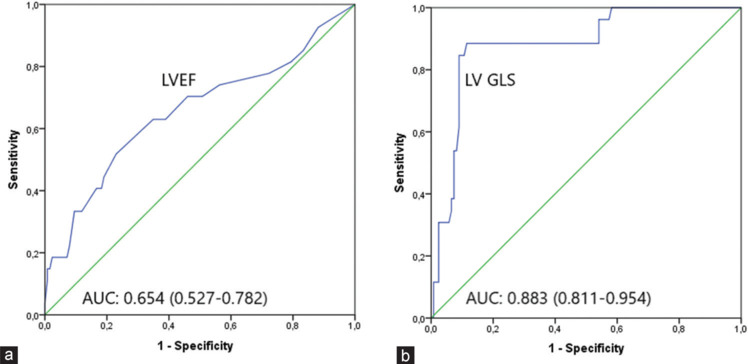
Results: Out of 153 patients, 17.8% showed disease progression. Receiver operating characteristic curves identified GLS as the most accurate predictor for clinical progression (area under the curve [AUC]: 0.883 (95% confidence interval [CI]: 0.811-0.954), cutoff: -9.0%, sensitivity: 88.5%, and specificity: 88.5%). LVEF performed less precisely (AUC: 0.654 [95% CI: 0.527-0.782], cutoff: 42%, sensitivity: 70.4%, and specificity: 54%). Depressed GLS was a strong and significant predictor for disease progression (hazard ratio [HR]: 16.7 (95% CI: 6.2-35.1), P < 0.001). Reduced LVEF showed to be a less reliable predictor (HR: 2.4 [95% CI: 1.1-5.2]).
Conclusions: GLS reliably predicts clinical progression in asymptomatic stable HF patients, with greater accuracy than LVEF. Its implementation in the risk stratification of these patients could help to identify those patients who are at greatest risk and may benefit from an intensification of their follow up and/or HF treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


