Daniel Bello, Megan Jones, Ishaan Gadiyar, Laura Artim, Sophia H Blyth, Roscoe O Brady, Simon Vandekar, Heather Burrell Ward
{"title":"经颅磁刺激的症状激发和临床反应:系统回顾和荟萃分析。","authors":"Daniel Bello, Megan Jones, Ishaan Gadiyar, Laura Artim, Sophia H Blyth, Roscoe O Brady, Simon Vandekar, Heather Burrell Ward","doi":"10.1001/jamapsychiatry.2025.0792","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Transcranial magnetic stimulation (TMS), a form of noninvasive brain stimulation used to treat major depressive disorder, obsessive-compulsive disorder (OCD), and nicotine dependence, has well-established state-dependent effects on brain circuitry. However, a major question for TMS remains: does brain state affect clinical response?</p><p><strong>Objective: </strong>To quantify the association between symptom provocation and clinical response to TMS for OCD and nicotine dependence, the only Food and Drug Administration-cleared TMS indications with symptom provocation.</p><p><strong>Data sources: </strong>PubMed, CINAHL, Embase, PsycInfo until August 30, 2024.</p><p><strong>Study selection: </strong>Randomized clinical trials of TMS for OCD or nicotine dependence with a clinical outcome. Of 600 studies identified, 71 met inclusion criteria.</p><p><strong>Data extraction and synthesis: </strong>Data extraction was completed independently by 2 extractors and cross-checked by a third. Standardized mean difference (SMD) and SE were estimated via Hedges g and synthesized data in a 3-level random-effects meta-analysis. Study data were analyzed from August 2023 to March 2025.</p><p><strong>Main outcomes and measures: </strong>Primary outcomes were clinical response measures.</p><p><strong>Results: </strong>A total of 71 studies met inclusion criteria and included 3246 participants (mean [SD] age; 37.8 [8.0] years; mean [SD] percentage female, 44.1% [17.2%]). Included in the meta-analysis were 63 studies with 2998 participants. For OCD studies, active TMS was associated with better clinical response than sham both with (SMD = -0.51; 95% CI, -0.96 to -0.07; P = 0.04) and without (SMD = -0.29; 95% CI, -0.40 to -0.17; P < .001) symptom provocation. For nicotine use, active TMS was associated with better clinical response than sham when used with (SMD = -0.56; 95% CI, -1.12 to 0; P = .05) but not without (SMD = -0.35; 95% CI, -0.74 to 0.04; P = .08) symptom provocation. For OCD studies, the estimated expected added effect of provocation was SMD of -0.22 (95% CI, -0.65 to 0.20; P = .22). In nicotine studies, the estimated expected added effect of provocation was SMD of -0.21 (95% CI, -1.00 to 0.58; P = .57).</p><p><strong>Conclusions and relevance: </strong>Results of this systematic review and meta-analysis suggest that symptom provocation may enhance clinical response to TMS for OCD and nicotine dependence. Studies comparing TMS with and without provocation are critical to establish the causal effect of provocation.</p>","PeriodicalId":14800,"journal":{"name":"JAMA Psychiatry","volume":" ","pages":"768-777"},"PeriodicalIF":17.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138803/pdf/","citationCount":"0","resultStr":"{\"title\":\"Symptom Provocation and Clinical Response to Transcranial Magnetic Stimulation: A Systematic Review and Meta-Analysis.\",\"authors\":\"Daniel Bello, Megan Jones, Ishaan Gadiyar, Laura Artim, Sophia H Blyth, Roscoe O Brady, Simon Vandekar, Heather Burrell Ward\",\"doi\":\"10.1001/jamapsychiatry.2025.0792\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Transcranial magnetic stimulation (TMS), a form of noninvasive brain stimulation used to treat major depressive disorder, obsessive-compulsive disorder (OCD), and nicotine dependence, has well-established state-dependent effects on brain circuitry. However, a major question for TMS remains: does brain state affect clinical response?</p><p><strong>Objective: </strong>To quantify the association between symptom provocation and clinical response to TMS for OCD and nicotine dependence, the only Food and Drug Administration-cleared TMS indications with symptom provocation.</p><p><strong>Data sources: </strong>PubMed, CINAHL, Embase, PsycInfo until August 30, 2024.</p><p><strong>Study selection: </strong>Randomized clinical trials of TMS for OCD or nicotine dependence with a clinical outcome. Of 600 studies identified, 71 met inclusion criteria.</p><p><strong>Data extraction and synthesis: </strong>Data extraction was completed independently by 2 extractors and cross-checked by a third. Standardized mean difference (SMD) and SE were estimated via Hedges g and synthesized data in a 3-level random-effects meta-analysis. Study data were analyzed from August 2023 to March 2025.</p><p><strong>Main outcomes and measures: </strong>Primary outcomes were clinical response measures.</p><p><strong>Results: </strong>A total of 71 studies met inclusion criteria and included 3246 participants (mean [SD] age; 37.8 [8.0] years; mean [SD] percentage female, 44.1% [17.2%]). Included in the meta-analysis were 63 studies with 2998 participants. For OCD studies, active TMS was associated with better clinical response than sham both with (SMD = -0.51; 95% CI, -0.96 to -0.07; P = 0.04) and without (SMD = -0.29; 95% CI, -0.40 to -0.17; P < .001) symptom provocation. For nicotine use, active TMS was associated with better clinical response than sham when used with (SMD = -0.56; 95% CI, -1.12 to 0; P = .05) but not without (SMD = -0.35; 95% CI, -0.74 to 0.04; P = .08) symptom provocation. For OCD studies, the estimated expected added effect of provocation was SMD of -0.22 (95% CI, -0.65 to 0.20; P = .22). In nicotine studies, the estimated expected added effect of provocation was SMD of -0.21 (95% CI, -1.00 to 0.58; P = .57).</p><p><strong>Conclusions and relevance: </strong>Results of this systematic review and meta-analysis suggest that symptom provocation may enhance clinical response to TMS for OCD and nicotine dependence. Studies comparing TMS with and without provocation are critical to establish the causal effect of provocation.</p>\",\"PeriodicalId\":14800,\"journal\":{\"name\":\"JAMA Psychiatry\",\"volume\":\" \",\"pages\":\"768-777\"},\"PeriodicalIF\":17.1000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138803/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Psychiatry\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamapsychiatry.2025.0792\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamapsychiatry.2025.0792","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Symptom Provocation and Clinical Response to Transcranial Magnetic Stimulation: A Systematic Review and Meta-Analysis.
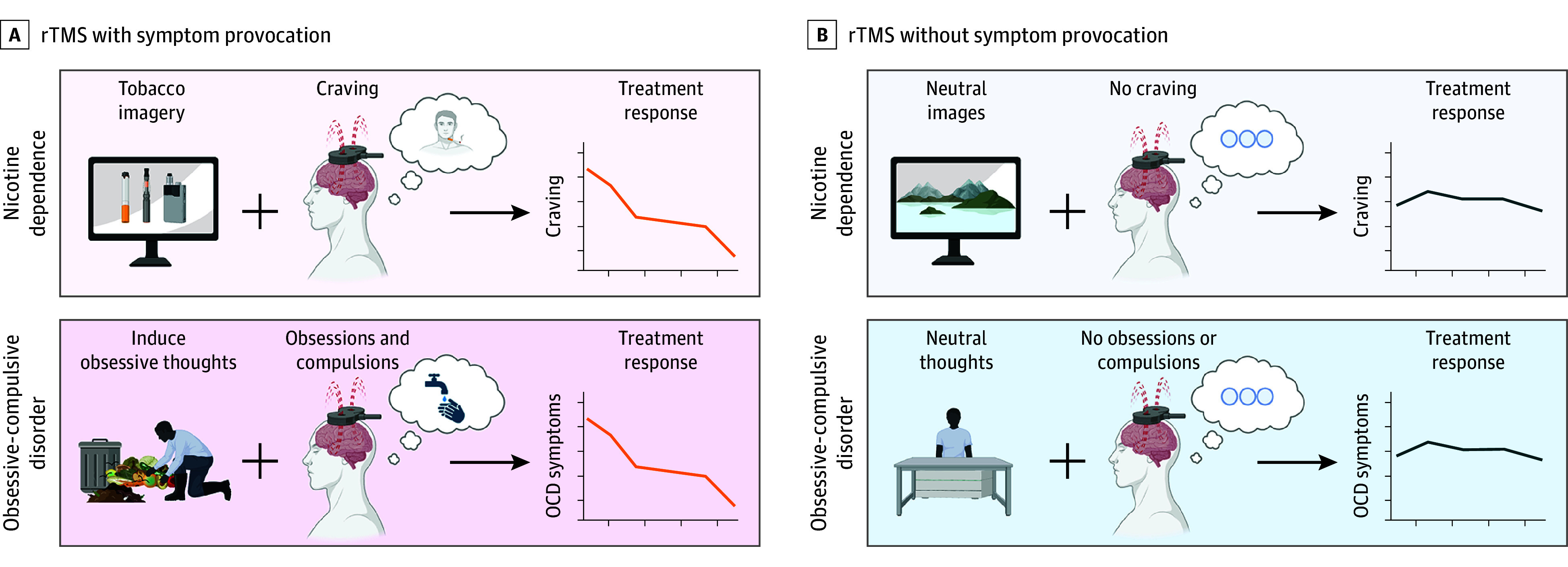
Importance: Transcranial magnetic stimulation (TMS), a form of noninvasive brain stimulation used to treat major depressive disorder, obsessive-compulsive disorder (OCD), and nicotine dependence, has well-established state-dependent effects on brain circuitry. However, a major question for TMS remains: does brain state affect clinical response?
Objective: To quantify the association between symptom provocation and clinical response to TMS for OCD and nicotine dependence, the only Food and Drug Administration-cleared TMS indications with symptom provocation.
Data sources: PubMed, CINAHL, Embase, PsycInfo until August 30, 2024.
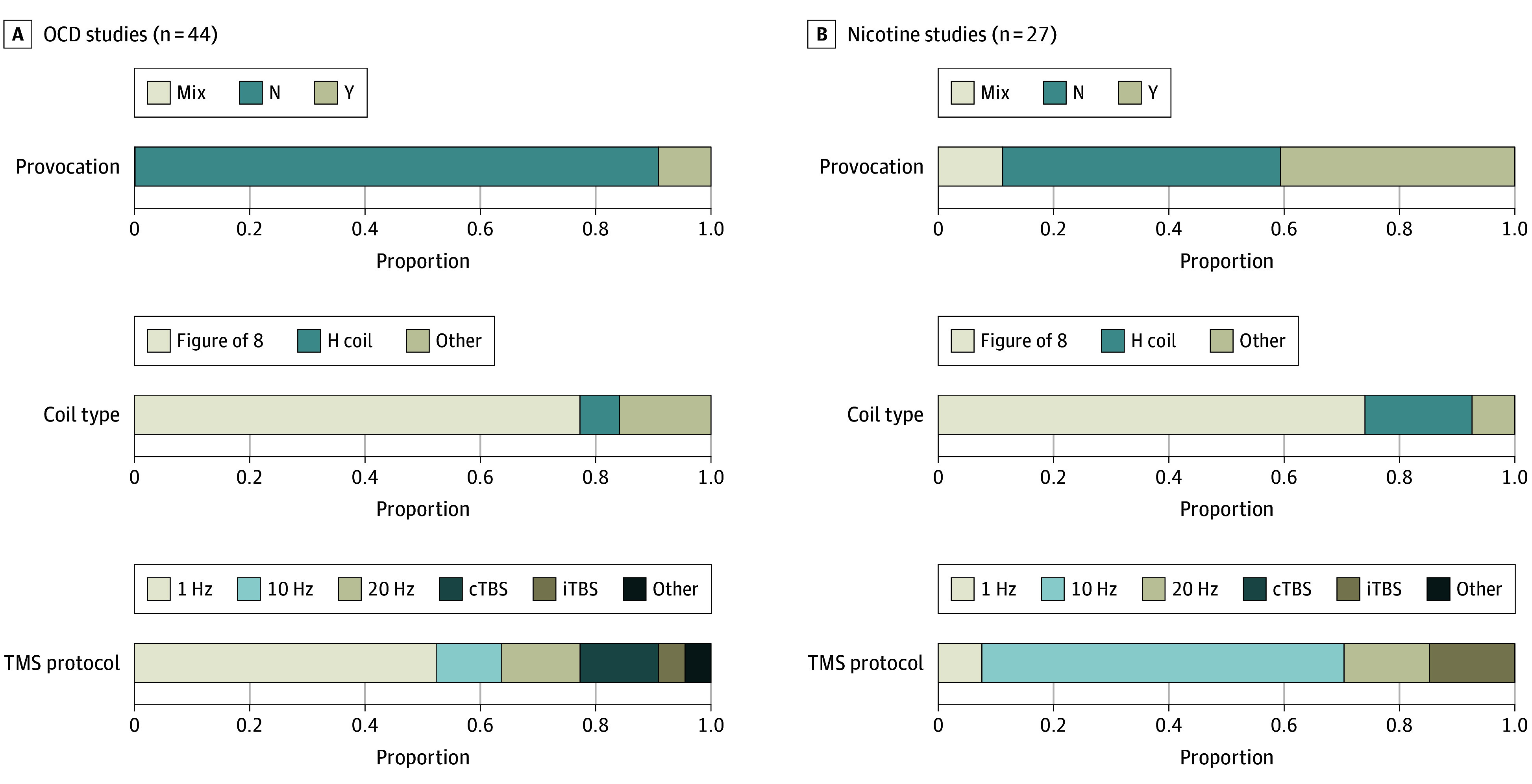
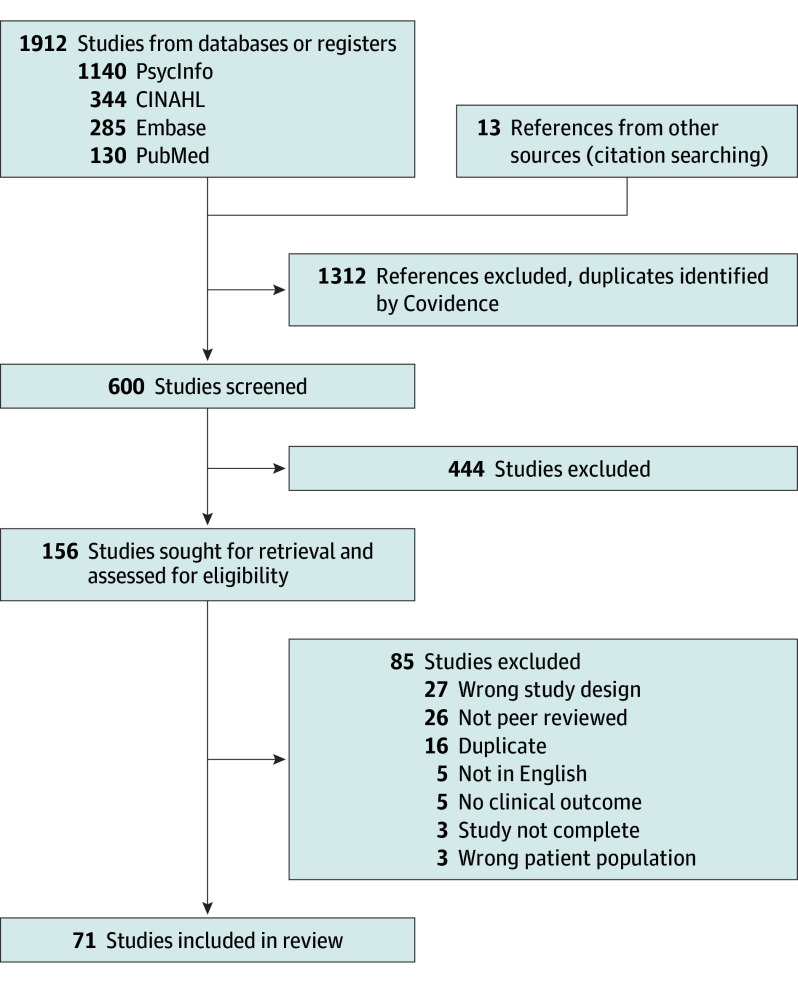
Study selection: Randomized clinical trials of TMS for OCD or nicotine dependence with a clinical outcome. Of 600 studies identified, 71 met inclusion criteria.
Data extraction and synthesis: Data extraction was completed independently by 2 extractors and cross-checked by a third. Standardized mean difference (SMD) and SE were estimated via Hedges g and synthesized data in a 3-level random-effects meta-analysis. Study data were analyzed from August 2023 to March 2025.
Main outcomes and measures: Primary outcomes were clinical response measures.
Results: A total of 71 studies met inclusion criteria and included 3246 participants (mean [SD] age; 37.8 [8.0] years; mean [SD] percentage female, 44.1% [17.2%]). Included in the meta-analysis were 63 studies with 2998 participants. For OCD studies, active TMS was associated with better clinical response than sham both with (SMD = -0.51; 95% CI, -0.96 to -0.07; P = 0.04) and without (SMD = -0.29; 95% CI, -0.40 to -0.17; P < .001) symptom provocation. For nicotine use, active TMS was associated with better clinical response than sham when used with (SMD = -0.56; 95% CI, -1.12 to 0; P = .05) but not without (SMD = -0.35; 95% CI, -0.74 to 0.04; P = .08) symptom provocation. For OCD studies, the estimated expected added effect of provocation was SMD of -0.22 (95% CI, -0.65 to 0.20; P = .22). In nicotine studies, the estimated expected added effect of provocation was SMD of -0.21 (95% CI, -1.00 to 0.58; P = .57).
Conclusions and relevance: Results of this systematic review and meta-analysis suggest that symptom provocation may enhance clinical response to TMS for OCD and nicotine dependence. Studies comparing TMS with and without provocation are critical to establish the causal effect of provocation.
期刊介绍:
JAMA Psychiatry is a global, peer-reviewed journal catering to clinicians, scholars, and research scientists in psychiatry, mental health, behavioral science, and related fields. The Archives of Neurology & Psychiatry originated in 1919, splitting into two journals in 1959: Archives of Neurology and Archives of General Psychiatry. In 2013, these evolved into JAMA Neurology and JAMA Psychiatry, respectively. JAMA Psychiatry is affiliated with the JAMA Network, a group of peer-reviewed medical and specialty publications.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


