Christian Otte, Woo Ri Chae, Deniz Yildirim Dogan, Dominique Piber, Stefan Roepke, An Bin Cho, Samuel Trumm, Michael Kaczmarczyk, Jelena Brasanac, Katja Wingenfeld, Stefanie Koglin, Johannes Wieditz, Klaus Junghanns, Michael Lucht, David Prvulovic, Tillmann H C Krüger, Jan Terock, Moritz Haaf, Tobias Hofmann, Nicole Mauche, Jan Philipp Klein, Hans Jörgen Grabe, Andreas Reif, Kai G Kahl, Deborah Janowitz, Gregor Leicht, Kim Hinkelmann, Maria Strauß, Tim Friede, Stefan M Gold
{"title":"辛伐他汀作为艾司西酞普兰治疗重度抑郁症和肥胖症患者的附加治疗:一项随机临床试验。","authors":"Christian Otte, Woo Ri Chae, Deniz Yildirim Dogan, Dominique Piber, Stefan Roepke, An Bin Cho, Samuel Trumm, Michael Kaczmarczyk, Jelena Brasanac, Katja Wingenfeld, Stefanie Koglin, Johannes Wieditz, Klaus Junghanns, Michael Lucht, David Prvulovic, Tillmann H C Krüger, Jan Terock, Moritz Haaf, Tobias Hofmann, Nicole Mauche, Jan Philipp Klein, Hans Jörgen Grabe, Andreas Reif, Kai G Kahl, Deborah Janowitz, Gregor Leicht, Kim Hinkelmann, Maria Strauß, Tim Friede, Stefan M Gold","doi":"10.1001/jamapsychiatry.2025.0801","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Major depressive disorder (MDD) and obesity are common noncommunicable disorders associated with substantial disease burden, which frequently occur comorbidly. Intriguingly, converging lines of evidence from animal models and genetic and observational studies have suggested a biological link between obesity, metabolic syndrome, and depression. Several small randomized clinical trials (RCTs) have suggested the antidepressive potential of statins.</p><p><strong>Objective: </strong>To examine whether simvastatin added to escitalopram is efficacious in improving depressive symptoms compared with add-on placebo.</p><p><strong>Design, setting, and participants: </strong>This was a confirmatory, double-blind, placebo-controlled, multicenter RCT. Adults with MDD and comorbid obesity from 9 tertiary care settings in Germany were enrolled in this analysis. Data were analyzed from July to October 2024.</p><p><strong>Interventions: </strong>Simvastatin (40 mg per day) or placebo as add-on to escitalopram (10 mg for the first 2 weeks, then increased to 20 mg until the end of study) in a double-blind fashion for 12 weeks.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was change in Montgomery-Åsberg Depression Rating Scale (MADRS) score from baseline (week 0) to week 12.</p><p><strong>Results: </strong>From August 21, 2020, to June 06, 2024, a total of 161 patients were enrolled at 9 sites in Germany, of which 160 patients were included in the intention-to-treat analysis (placebo: n = 79, simvastatin: n = 81; mean [SD] age, 39.0 [11.0] years; 126 female [79%]). Retention in the trial was excellent (95.6%), and blinding was effectively maintained. There were 4 serious adverse events with no difference between the groups. Primary end point analysis in the intention-to-treat sample showed no significant treatment effect of add-on simvastatin in MADRS scores (mixed models for repeated measures least squares mean difference, 0.47 points; 95% CI, -2.08 to 3.02; P = .71). No effects of simvastatin treatment were observed in any of the mental health-related secondary end points. However, simvastatin treatment significantly reduced low-density lipoprotein cholesterol (simvastatin, -40.37 mg/dL; 95% CI, -47.41 to -33.33 mg/dL; placebo, -3.78 mg/dL; 95% CI, -11.18 to 3.62 mg/dL; P < .001), total cholesterol (simvastatin, -39.07 mg/dL; 95% CI, -49.42 to -28.73 mg/dL; placebo, -4.89 mg/dL; 95% CI, -15.64 to 5.87 mg/dL; P < .001), and C-reactive protein (simvastatin, -1.04 mg/L; 95% CI, -1.89 to -0.20 mg/L; placebo, 0.57 mg/L; 95% CI, -0.28 to 1.42 mg/L; P = .003) compared with placebo.</p><p><strong>Conclusions and relevance: </strong>The study failed to meet its primary end point. This demonstrates that simvastatin did not exert additional antidepressive effects when added to escitalopram in patients with comorbid MDD and obesity, despite improving the cardiovascular risk profile.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT04301271.</p>","PeriodicalId":14800,"journal":{"name":"JAMA Psychiatry","volume":" ","pages":"759-767"},"PeriodicalIF":17.1000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138799/pdf/","citationCount":"0","resultStr":"{\"title\":\"Simvastatin as Add-On Treatment to Escitalopram in Patients With Major Depression and Obesity: A Randomized Clinical Trial.\",\"authors\":\"Christian Otte, Woo Ri Chae, Deniz Yildirim Dogan, Dominique Piber, Stefan Roepke, An Bin Cho, Samuel Trumm, Michael Kaczmarczyk, Jelena Brasanac, Katja Wingenfeld, Stefanie Koglin, Johannes Wieditz, Klaus Junghanns, Michael Lucht, David Prvulovic, Tillmann H C Krüger, Jan Terock, Moritz Haaf, Tobias Hofmann, Nicole Mauche, Jan Philipp Klein, Hans Jörgen Grabe, Andreas Reif, Kai G Kahl, Deborah Janowitz, Gregor Leicht, Kim Hinkelmann, Maria Strauß, Tim Friede, Stefan M Gold\",\"doi\":\"10.1001/jamapsychiatry.2025.0801\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Importance: </strong>Major depressive disorder (MDD) and obesity are common noncommunicable disorders associated with substantial disease burden, which frequently occur comorbidly. Intriguingly, converging lines of evidence from animal models and genetic and observational studies have suggested a biological link between obesity, metabolic syndrome, and depression. Several small randomized clinical trials (RCTs) have suggested the antidepressive potential of statins.</p><p><strong>Objective: </strong>To examine whether simvastatin added to escitalopram is efficacious in improving depressive symptoms compared with add-on placebo.</p><p><strong>Design, setting, and participants: </strong>This was a confirmatory, double-blind, placebo-controlled, multicenter RCT. Adults with MDD and comorbid obesity from 9 tertiary care settings in Germany were enrolled in this analysis. Data were analyzed from July to October 2024.</p><p><strong>Interventions: </strong>Simvastatin (40 mg per day) or placebo as add-on to escitalopram (10 mg for the first 2 weeks, then increased to 20 mg until the end of study) in a double-blind fashion for 12 weeks.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was change in Montgomery-Åsberg Depression Rating Scale (MADRS) score from baseline (week 0) to week 12.</p><p><strong>Results: </strong>From August 21, 2020, to June 06, 2024, a total of 161 patients were enrolled at 9 sites in Germany, of which 160 patients were included in the intention-to-treat analysis (placebo: n = 79, simvastatin: n = 81; mean [SD] age, 39.0 [11.0] years; 126 female [79%]). Retention in the trial was excellent (95.6%), and blinding was effectively maintained. There were 4 serious adverse events with no difference between the groups. Primary end point analysis in the intention-to-treat sample showed no significant treatment effect of add-on simvastatin in MADRS scores (mixed models for repeated measures least squares mean difference, 0.47 points; 95% CI, -2.08 to 3.02; P = .71). No effects of simvastatin treatment were observed in any of the mental health-related secondary end points. However, simvastatin treatment significantly reduced low-density lipoprotein cholesterol (simvastatin, -40.37 mg/dL; 95% CI, -47.41 to -33.33 mg/dL; placebo, -3.78 mg/dL; 95% CI, -11.18 to 3.62 mg/dL; P < .001), total cholesterol (simvastatin, -39.07 mg/dL; 95% CI, -49.42 to -28.73 mg/dL; placebo, -4.89 mg/dL; 95% CI, -15.64 to 5.87 mg/dL; P < .001), and C-reactive protein (simvastatin, -1.04 mg/L; 95% CI, -1.89 to -0.20 mg/L; placebo, 0.57 mg/L; 95% CI, -0.28 to 1.42 mg/L; P = .003) compared with placebo.</p><p><strong>Conclusions and relevance: </strong>The study failed to meet its primary end point. This demonstrates that simvastatin did not exert additional antidepressive effects when added to escitalopram in patients with comorbid MDD and obesity, despite improving the cardiovascular risk profile.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifier: NCT04301271.</p>\",\"PeriodicalId\":14800,\"journal\":{\"name\":\"JAMA Psychiatry\",\"volume\":\" \",\"pages\":\"759-767\"},\"PeriodicalIF\":17.1000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12138799/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JAMA Psychiatry\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1001/jamapsychiatry.2025.0801\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PSYCHIATRY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamapsychiatry.2025.0801","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
Simvastatin as Add-On Treatment to Escitalopram in Patients With Major Depression and Obesity: A Randomized Clinical Trial.
Importance: Major depressive disorder (MDD) and obesity are common noncommunicable disorders associated with substantial disease burden, which frequently occur comorbidly. Intriguingly, converging lines of evidence from animal models and genetic and observational studies have suggested a biological link between obesity, metabolic syndrome, and depression. Several small randomized clinical trials (RCTs) have suggested the antidepressive potential of statins.
Objective: To examine whether simvastatin added to escitalopram is efficacious in improving depressive symptoms compared with add-on placebo.
Design, setting, and participants: This was a confirmatory, double-blind, placebo-controlled, multicenter RCT. Adults with MDD and comorbid obesity from 9 tertiary care settings in Germany were enrolled in this analysis. Data were analyzed from July to October 2024.
Interventions: Simvastatin (40 mg per day) or placebo as add-on to escitalopram (10 mg for the first 2 weeks, then increased to 20 mg until the end of study) in a double-blind fashion for 12 weeks.
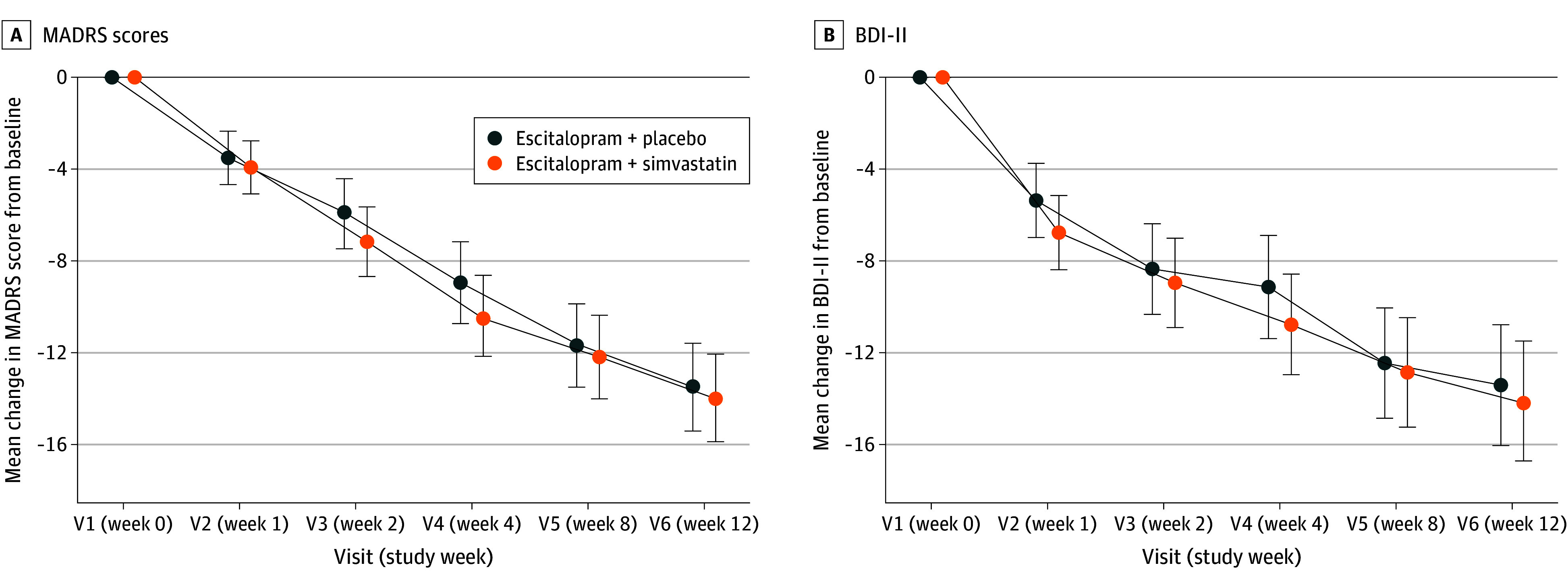
Main outcomes and measures: The primary outcome was change in Montgomery-Åsberg Depression Rating Scale (MADRS) score from baseline (week 0) to week 12.
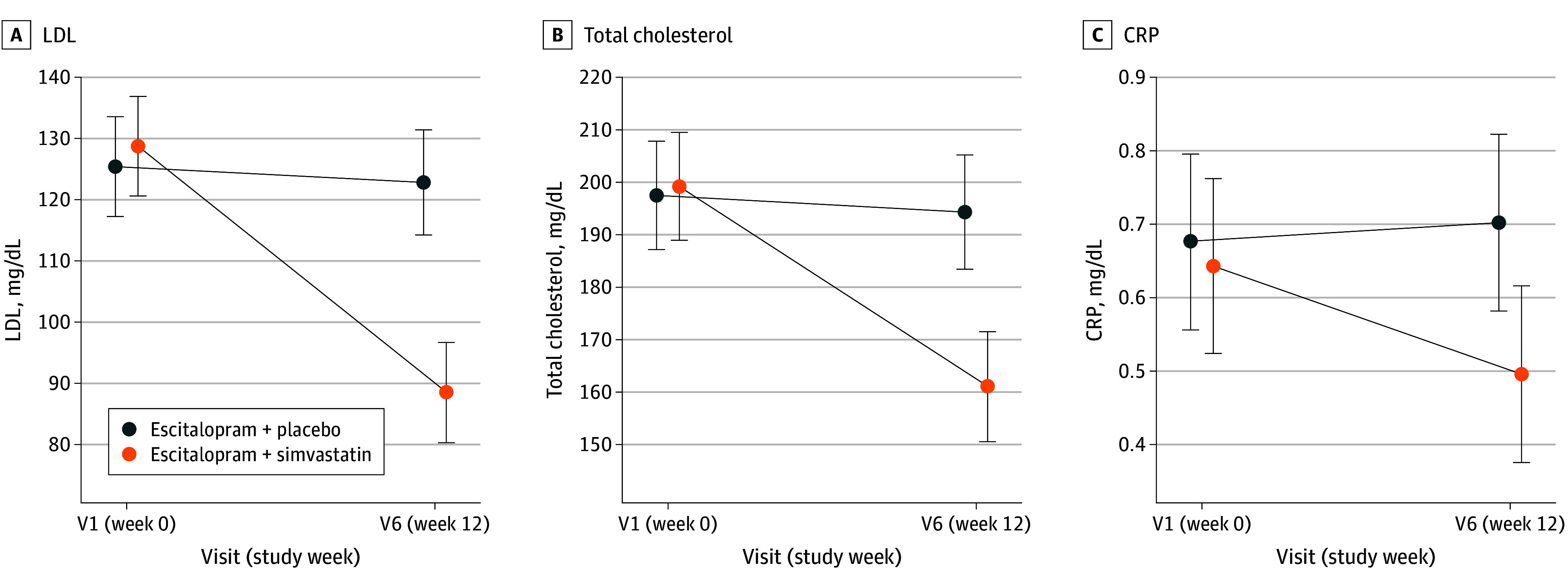
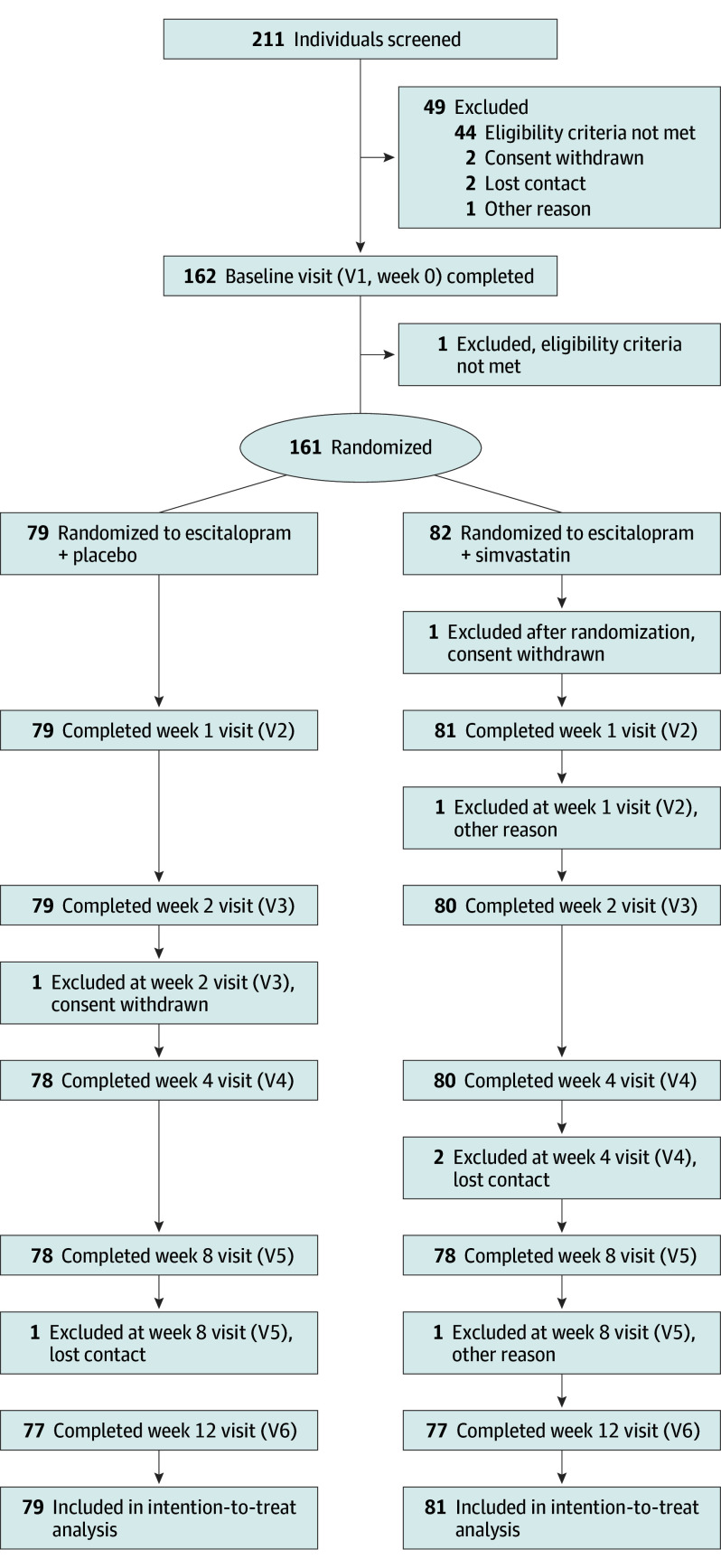
Results: From August 21, 2020, to June 06, 2024, a total of 161 patients were enrolled at 9 sites in Germany, of which 160 patients were included in the intention-to-treat analysis (placebo: n = 79, simvastatin: n = 81; mean [SD] age, 39.0 [11.0] years; 126 female [79%]). Retention in the trial was excellent (95.6%), and blinding was effectively maintained. There were 4 serious adverse events with no difference between the groups. Primary end point analysis in the intention-to-treat sample showed no significant treatment effect of add-on simvastatin in MADRS scores (mixed models for repeated measures least squares mean difference, 0.47 points; 95% CI, -2.08 to 3.02; P = .71). No effects of simvastatin treatment were observed in any of the mental health-related secondary end points. However, simvastatin treatment significantly reduced low-density lipoprotein cholesterol (simvastatin, -40.37 mg/dL; 95% CI, -47.41 to -33.33 mg/dL; placebo, -3.78 mg/dL; 95% CI, -11.18 to 3.62 mg/dL; P < .001), total cholesterol (simvastatin, -39.07 mg/dL; 95% CI, -49.42 to -28.73 mg/dL; placebo, -4.89 mg/dL; 95% CI, -15.64 to 5.87 mg/dL; P < .001), and C-reactive protein (simvastatin, -1.04 mg/L; 95% CI, -1.89 to -0.20 mg/L; placebo, 0.57 mg/L; 95% CI, -0.28 to 1.42 mg/L; P = .003) compared with placebo.
Conclusions and relevance: The study failed to meet its primary end point. This demonstrates that simvastatin did not exert additional antidepressive effects when added to escitalopram in patients with comorbid MDD and obesity, despite improving the cardiovascular risk profile.
期刊介绍:
JAMA Psychiatry is a global, peer-reviewed journal catering to clinicians, scholars, and research scientists in psychiatry, mental health, behavioral science, and related fields. The Archives of Neurology & Psychiatry originated in 1919, splitting into two journals in 1959: Archives of Neurology and Archives of General Psychiatry. In 2013, these evolved into JAMA Neurology and JAMA Psychiatry, respectively. JAMA Psychiatry is affiliated with the JAMA Network, a group of peer-reviewed medical and specialty publications.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


