Corey Fang, Casey Dobie, Amita Ketkar, Monica Verduzco-Gutierrez, George Fadda, Claire Bocage, Chia Chen Jenny Teng, Raven Perez, Mark Brunk-Grady, Lisa Glasser, Christine Dube, Nadine Breslin, Vincent Willey
{"title":"评估年龄和合并症对COVID-19结局和医疗费用的影响:美国免疫功能低下人群和普通人群(EON-US)的比较分析","authors":"Corey Fang, Casey Dobie, Amita Ketkar, Monica Verduzco-Gutierrez, George Fadda, Claire Bocage, Chia Chen Jenny Teng, Raven Perez, Mark Brunk-Grady, Lisa Glasser, Christine Dube, Nadine Breslin, Vincent Willey","doi":"10.1007/s40121-025-01160-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The COVID-19 public health emergency (PHE) ended in May 2023, but limited information exists on the continued risk of severe COVID-19 among the immunocompromised (IC) population and those with certain chronic medical conditions (CMCs). This study aimed to assess the risk of moderate/severe COVID-19 and compare associated healthcare resource utilization (HCRU) and costs for IC vs. general populations, with a focus on increasing age and CMC burden in the IC population.</p><p><strong>Methods: </strong>This retrospective observational cohort study analyzed claims from the Healthcare Integrated Research Database (HIRD<sup>®</sup>) for individuals with a COVID-19 diagnosis or positive test between March 2023 and February 2024. Patients were followed until the study's end, disenrollment, or death. Propensity scores were calculated using binomial logistic regression to adjust for confounding when comparing the IC and general population groups. The IC cohort was divided into five subgroups based on age (</≥ 65 years) and number of CMCs (1, 2, or 3 +).</p><p><strong>Results: </strong>The IC cohort (N = 8025) was older and had a higher comorbidity burden than the general population (N = 458,163), which was balanced after matching (N = 7410 each). The IC cohort had a significantly higher rate of severe COVID-19 vs. the general population (9.5% vs. 1.1%; p < 0.001), but there was no difference after matching (8.9% vs. 8.7%; p = 0.772). Older age and increasing number of CMCs led to a significantly higher proportion of severe COVID-19. Compared to the general population, the IC cohort had significantly higher inpatient all-cause and COVID-19-related HCRU and costs, except within the matched analysis where COVID-19-related hospitalizations were not significantly different between the groups.</p><p><strong>Conclusions: </strong>Severe COVID-19 continued to disproportionately affect IC individuals after the PHE was lifted. Additionally, our matched results identified a subset of the general population with high baseline comorbidity burden and risk similar to the matched IC cohort for severe COVID-19.</p>","PeriodicalId":13592,"journal":{"name":"Infectious Diseases and Therapy","volume":" ","pages":"1343-1367"},"PeriodicalIF":5.3000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151973/pdf/","citationCount":"0","resultStr":"{\"title\":\"Evaluating the Impact of Age and Comorbidities on COVID-19 Outcomes and Healthcare Costs: A Comparative Analysis of Immunocompromised and General Populations in the United States (EON-US).\",\"authors\":\"Corey Fang, Casey Dobie, Amita Ketkar, Monica Verduzco-Gutierrez, George Fadda, Claire Bocage, Chia Chen Jenny Teng, Raven Perez, Mark Brunk-Grady, Lisa Glasser, Christine Dube, Nadine Breslin, Vincent Willey\",\"doi\":\"10.1007/s40121-025-01160-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The COVID-19 public health emergency (PHE) ended in May 2023, but limited information exists on the continued risk of severe COVID-19 among the immunocompromised (IC) population and those with certain chronic medical conditions (CMCs). This study aimed to assess the risk of moderate/severe COVID-19 and compare associated healthcare resource utilization (HCRU) and costs for IC vs. general populations, with a focus on increasing age and CMC burden in the IC population.</p><p><strong>Methods: </strong>This retrospective observational cohort study analyzed claims from the Healthcare Integrated Research Database (HIRD<sup>®</sup>) for individuals with a COVID-19 diagnosis or positive test between March 2023 and February 2024. Patients were followed until the study's end, disenrollment, or death. Propensity scores were calculated using binomial logistic regression to adjust for confounding when comparing the IC and general population groups. The IC cohort was divided into five subgroups based on age (</≥ 65 years) and number of CMCs (1, 2, or 3 +).</p><p><strong>Results: </strong>The IC cohort (N = 8025) was older and had a higher comorbidity burden than the general population (N = 458,163), which was balanced after matching (N = 7410 each). The IC cohort had a significantly higher rate of severe COVID-19 vs. the general population (9.5% vs. 1.1%; p < 0.001), but there was no difference after matching (8.9% vs. 8.7%; p = 0.772). Older age and increasing number of CMCs led to a significantly higher proportion of severe COVID-19. Compared to the general population, the IC cohort had significantly higher inpatient all-cause and COVID-19-related HCRU and costs, except within the matched analysis where COVID-19-related hospitalizations were not significantly different between the groups.</p><p><strong>Conclusions: </strong>Severe COVID-19 continued to disproportionately affect IC individuals after the PHE was lifted. Additionally, our matched results identified a subset of the general population with high baseline comorbidity burden and risk similar to the matched IC cohort for severe COVID-19.</p>\",\"PeriodicalId\":13592,\"journal\":{\"name\":\"Infectious Diseases and Therapy\",\"volume\":\" \",\"pages\":\"1343-1367\"},\"PeriodicalIF\":5.3000,\"publicationDate\":\"2025-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12151973/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Diseases and Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40121-025-01160-z\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Diseases and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40121-025-01160-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Evaluating the Impact of Age and Comorbidities on COVID-19 Outcomes and Healthcare Costs: A Comparative Analysis of Immunocompromised and General Populations in the United States (EON-US).
Introduction: The COVID-19 public health emergency (PHE) ended in May 2023, but limited information exists on the continued risk of severe COVID-19 among the immunocompromised (IC) population and those with certain chronic medical conditions (CMCs). This study aimed to assess the risk of moderate/severe COVID-19 and compare associated healthcare resource utilization (HCRU) and costs for IC vs. general populations, with a focus on increasing age and CMC burden in the IC population.
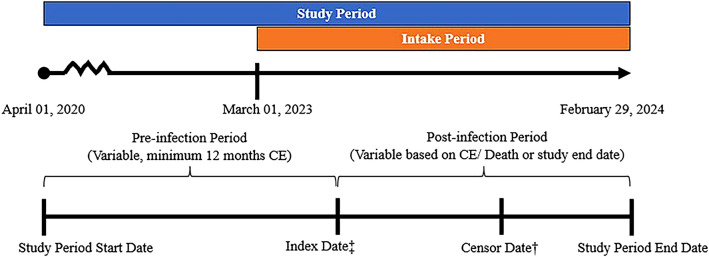
Methods: This retrospective observational cohort study analyzed claims from the Healthcare Integrated Research Database (HIRD®) for individuals with a COVID-19 diagnosis or positive test between March 2023 and February 2024. Patients were followed until the study's end, disenrollment, or death. Propensity scores were calculated using binomial logistic regression to adjust for confounding when comparing the IC and general population groups. The IC cohort was divided into five subgroups based on age (
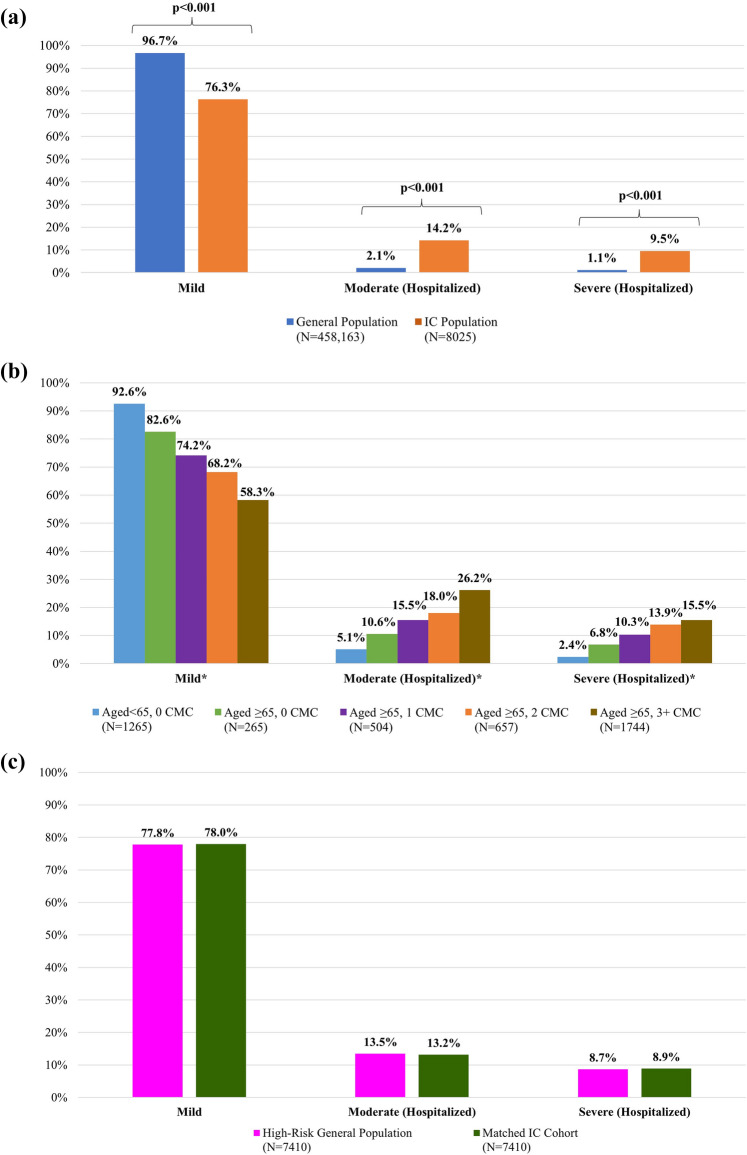
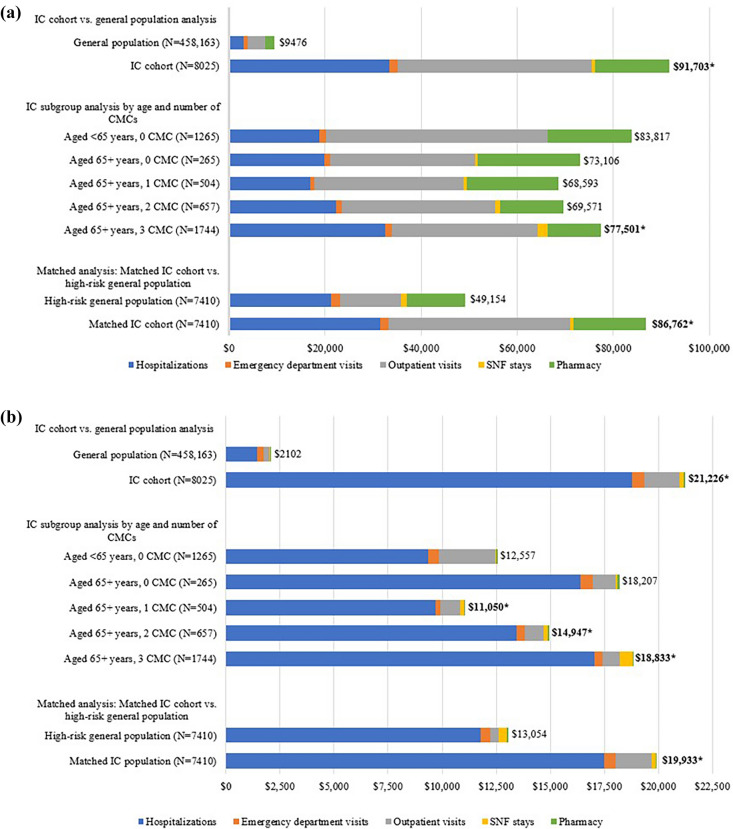
Results: The IC cohort (N = 8025) was older and had a higher comorbidity burden than the general population (N = 458,163), which was balanced after matching (N = 7410 each). The IC cohort had a significantly higher rate of severe COVID-19 vs. the general population (9.5% vs. 1.1%; p < 0.001), but there was no difference after matching (8.9% vs. 8.7%; p = 0.772). Older age and increasing number of CMCs led to a significantly higher proportion of severe COVID-19. Compared to the general population, the IC cohort had significantly higher inpatient all-cause and COVID-19-related HCRU and costs, except within the matched analysis where COVID-19-related hospitalizations were not significantly different between the groups.
Conclusions: Severe COVID-19 continued to disproportionately affect IC individuals after the PHE was lifted. Additionally, our matched results identified a subset of the general population with high baseline comorbidity burden and risk similar to the matched IC cohort for severe COVID-19.
期刊介绍:
Infectious Diseases and Therapy is an international, open access, peer-reviewed, rapid publication journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of infectious disease therapies and interventions, including vaccines and devices. Studies relating to diagnostic products and diagnosis, pharmacoeconomics, public health, epidemiology, quality of life, and patient care, management, and education are also encouraged.
Areas of focus include, but are not limited to, bacterial and fungal infections, viral infections (including HIV/AIDS and hepatitis), parasitological diseases, tuberculosis and other mycobacterial diseases, vaccinations and other interventions, and drug-resistance, chronic infections, epidemiology and tropical, emergent, pediatric, dermal and sexually-transmitted diseases.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


