{"title":"关于疼痛的教育和以认知为基础的干预经验不能减少医疗保健专业人员的慢性疼痛。","authors":"Asaf Weisman, Tomer Yona, Youssef Masharawi","doi":"10.7717/peerj.19448","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cognitive-based interventions like pain neuroscience education (PNE), cognitive behavioral therapy (CBT), acceptance commitment therapy (ACT), and mindfulness meditation are popular for managing chronic pain. Despite their widespread adoption, evidence for their efficacy remains contradictory. Healthcare professionals (HCPs) represent a unique population to evaluate these approaches, as they possess specialized knowledge about pain mechanisms and often implement these interventions with patients. The logical premise underlying cognitive-based interventions suggests that increased knowledge and cognitive engagement with pain concepts should reduce pain intensity, making educated HCPs with chronic pain an ideal test case for this theoretical framework.</p><p><strong>Purpose: </strong>To investigate whether HCPs with chronic pain who (HCPs+CP) are familiar with these methods experience less pain and improved quality of life compared to less experienced HCPs+CP and healthy HCPs (H-HCPs).</p><p><strong>Methods: </strong>This cross-sectional study used an anonymous online questionnaire distributed in English through closed professional social media groups internationally. Data were collected from 550 HCPs (319 healthy, 231 with chronic pain) primarily from Israel, Canada, United States, United Kingdom, and Australia. Participants were categorized by their knowledge of pain neuroscience, experience with cognitive-based interventions, and chronic pain type (primary or secondary). Pain intensity was measured using the Numerical Pain Rating Scale, and quality of life was assessed with the World Health Organization tool the WHOQOL-BREF. Statistical analyses included Spearman's correlation tests and independent samples t-tests.</p><p><strong>Results: </strong>Pain intensity did not significantly differ between primary pain group (4.24 ± 2.21) and secondary pain group (4.37 ± 2.33) (t = -0.267, <i>p</i> = 0.79, Cohen's d = -0.05). The total WHOQOL score was lower in HCPs+CP (66.81 ± 15.74) compared to healthy HCPs (71.13 ± 14.02) (t = -2.136, <i>p</i> = 0.035), but after removing respondents unfamiliar with interventions, no significant differences remained between groups across all WHOQOL domains (-0.09 < Cohen's d < 0.14, <i>p</i> > 0.05). Among the 146 H-HCPs who had recovered from chronic pain, only 11% attributed their recovery to cognitive-based interventions, while the majority credited physical therapy (37.7%) and spontaneous recovery (32.9%).</p><p><strong>Conclusion: </strong>Despite their specialized knowledge and experience with cognitive-based interventions, HCPs+CP did not report reduced pain intensity, though they maintained quality of life comparable to healthy colleagues. These findings challenge current theoretical models underlying cognitive-based pain management.</p>","PeriodicalId":19799,"journal":{"name":"PeerJ","volume":"13 ","pages":"e19448"},"PeriodicalIF":2.4000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12129007/pdf/","citationCount":"0","resultStr":"{\"title\":\"Education about pain and experience with cognitive-based interventions do not reduce healthcare professionals' chronic pain.\",\"authors\":\"Asaf Weisman, Tomer Yona, Youssef Masharawi\",\"doi\":\"10.7717/peerj.19448\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cognitive-based interventions like pain neuroscience education (PNE), cognitive behavioral therapy (CBT), acceptance commitment therapy (ACT), and mindfulness meditation are popular for managing chronic pain. Despite their widespread adoption, evidence for their efficacy remains contradictory. Healthcare professionals (HCPs) represent a unique population to evaluate these approaches, as they possess specialized knowledge about pain mechanisms and often implement these interventions with patients. The logical premise underlying cognitive-based interventions suggests that increased knowledge and cognitive engagement with pain concepts should reduce pain intensity, making educated HCPs with chronic pain an ideal test case for this theoretical framework.</p><p><strong>Purpose: </strong>To investigate whether HCPs with chronic pain who (HCPs+CP) are familiar with these methods experience less pain and improved quality of life compared to less experienced HCPs+CP and healthy HCPs (H-HCPs).</p><p><strong>Methods: </strong>This cross-sectional study used an anonymous online questionnaire distributed in English through closed professional social media groups internationally. Data were collected from 550 HCPs (319 healthy, 231 with chronic pain) primarily from Israel, Canada, United States, United Kingdom, and Australia. Participants were categorized by their knowledge of pain neuroscience, experience with cognitive-based interventions, and chronic pain type (primary or secondary). Pain intensity was measured using the Numerical Pain Rating Scale, and quality of life was assessed with the World Health Organization tool the WHOQOL-BREF. Statistical analyses included Spearman's correlation tests and independent samples t-tests.</p><p><strong>Results: </strong>Pain intensity did not significantly differ between primary pain group (4.24 ± 2.21) and secondary pain group (4.37 ± 2.33) (t = -0.267, <i>p</i> = 0.79, Cohen's d = -0.05). The total WHOQOL score was lower in HCPs+CP (66.81 ± 15.74) compared to healthy HCPs (71.13 ± 14.02) (t = -2.136, <i>p</i> = 0.035), but after removing respondents unfamiliar with interventions, no significant differences remained between groups across all WHOQOL domains (-0.09 < Cohen's d < 0.14, <i>p</i> > 0.05). Among the 146 H-HCPs who had recovered from chronic pain, only 11% attributed their recovery to cognitive-based interventions, while the majority credited physical therapy (37.7%) and spontaneous recovery (32.9%).</p><p><strong>Conclusion: </strong>Despite their specialized knowledge and experience with cognitive-based interventions, HCPs+CP did not report reduced pain intensity, though they maintained quality of life comparable to healthy colleagues. These findings challenge current theoretical models underlying cognitive-based pain management.</p>\",\"PeriodicalId\":19799,\"journal\":{\"name\":\"PeerJ\",\"volume\":\"13 \",\"pages\":\"e19448\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2025-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12129007/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PeerJ\",\"FirstCategoryId\":\"99\",\"ListUrlMain\":\"https://doi.org/10.7717/peerj.19448\",\"RegionNum\":3,\"RegionCategory\":\"生物学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MULTIDISCIPLINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PeerJ","FirstCategoryId":"99","ListUrlMain":"https://doi.org/10.7717/peerj.19448","RegionNum":3,"RegionCategory":"生物学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MULTIDISCIPLINARY SCIENCES","Score":null,"Total":0}
引用次数: 0
摘要
背景:基于认知的干预措施,如疼痛神经科学教育(PNE)、认知行为疗法(CBT)、接受承诺疗法(ACT)和正念冥想是治疗慢性疼痛的常用方法。尽管它们被广泛采用,但其有效性的证据仍然相互矛盾。医疗保健专业人员(HCPs)代表了一个独特的人群来评估这些方法,因为他们拥有关于疼痛机制的专业知识,并且经常对患者实施这些干预措施。基于认知干预的逻辑前提表明,增加对疼痛概念的知识和认知参与应该减少疼痛强度,使受过教育的慢性疼痛医护人员成为该理论框架的理想测试案例。目的:探讨熟悉这些方法的慢性疼痛HCPs (HCPs+CP)是否比没有经验的HCPs+CP和健康的HCPs (H-HCPs)更能减轻疼痛和改善生活质量。方法:本横断面研究采用匿名在线问卷,通过封闭的国际专业社交媒体团体以英语分发。数据收集自主要来自以色列、加拿大、美国、英国和澳大利亚的550名HCPs(319人健康,231人患有慢性疼痛)。参与者根据他们的疼痛神经科学知识、认知干预经验和慢性疼痛类型(原发性或继发性)进行分类。采用数值疼痛评定量表测量疼痛强度,采用世界卫生组织WHOQOL-BREF工具评估生活质量。统计分析包括Spearman相关检验和独立样本t检验。结果:原发性疼痛组(4.24±2.21)与继发性疼痛组(4.37±2.33)疼痛强度差异无统计学意义(t = -0.267, p = 0.79, Cohen’s d = -0.05)。健康HCPs的WHOQOL评分(71.13±14.02)低于健康HCPs(66.81±15.74)(t = -2.136, p = 0.035),但在剔除不熟悉干预措施的受访者后,各组间WHOQOL各域的差异无统计学意义(-0.09 < Cohen’s d < 0.14, p < 0.05)。在146名从慢性疼痛中恢复的H-HCPs中,只有11%将其恢复归因于基于认知的干预,而大多数归功于物理治疗(37.7%)和自发恢复(32.9%)。结论:尽管HCPs+CP具有认知干预方面的专业知识和经验,但他们并没有报告疼痛强度减轻,尽管他们保持了与健康同事相当的生活质量。这些发现挑战了当前基于认知的疼痛管理的理论模型。
Education about pain and experience with cognitive-based interventions do not reduce healthcare professionals' chronic pain.
Background: Cognitive-based interventions like pain neuroscience education (PNE), cognitive behavioral therapy (CBT), acceptance commitment therapy (ACT), and mindfulness meditation are popular for managing chronic pain. Despite their widespread adoption, evidence for their efficacy remains contradictory. Healthcare professionals (HCPs) represent a unique population to evaluate these approaches, as they possess specialized knowledge about pain mechanisms and often implement these interventions with patients. The logical premise underlying cognitive-based interventions suggests that increased knowledge and cognitive engagement with pain concepts should reduce pain intensity, making educated HCPs with chronic pain an ideal test case for this theoretical framework.
Purpose: To investigate whether HCPs with chronic pain who (HCPs+CP) are familiar with these methods experience less pain and improved quality of life compared to less experienced HCPs+CP and healthy HCPs (H-HCPs).
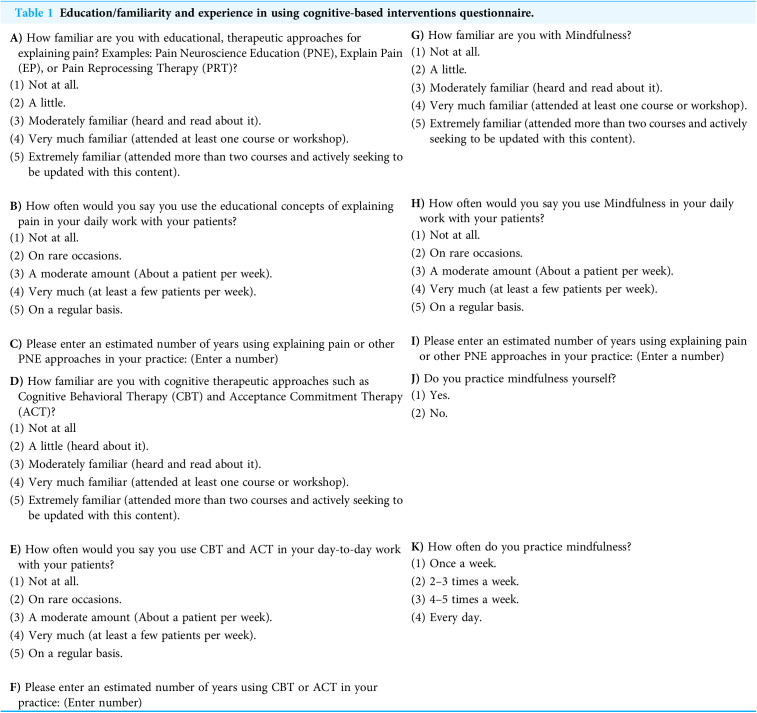
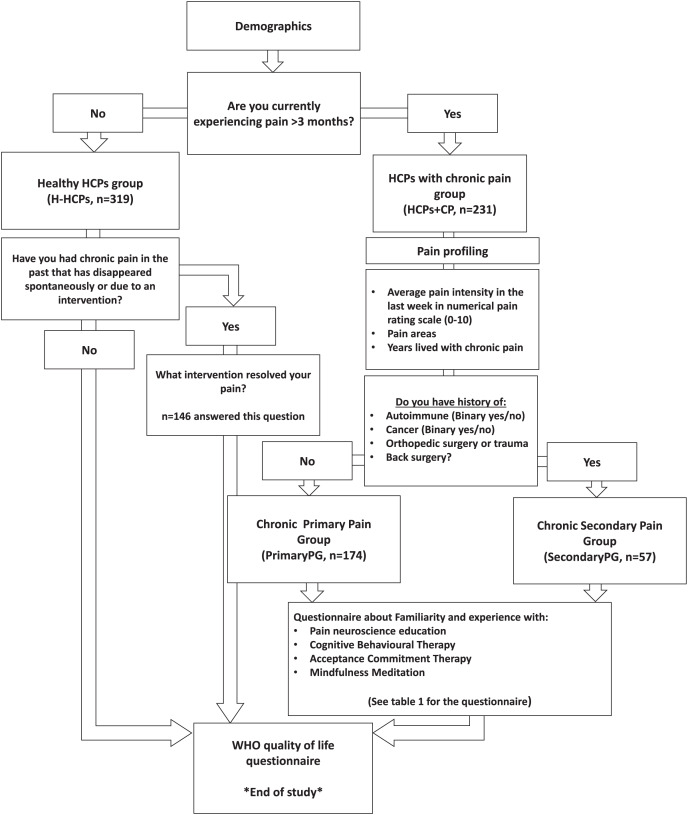
Methods: This cross-sectional study used an anonymous online questionnaire distributed in English through closed professional social media groups internationally. Data were collected from 550 HCPs (319 healthy, 231 with chronic pain) primarily from Israel, Canada, United States, United Kingdom, and Australia. Participants were categorized by their knowledge of pain neuroscience, experience with cognitive-based interventions, and chronic pain type (primary or secondary). Pain intensity was measured using the Numerical Pain Rating Scale, and quality of life was assessed with the World Health Organization tool the WHOQOL-BREF. Statistical analyses included Spearman's correlation tests and independent samples t-tests.
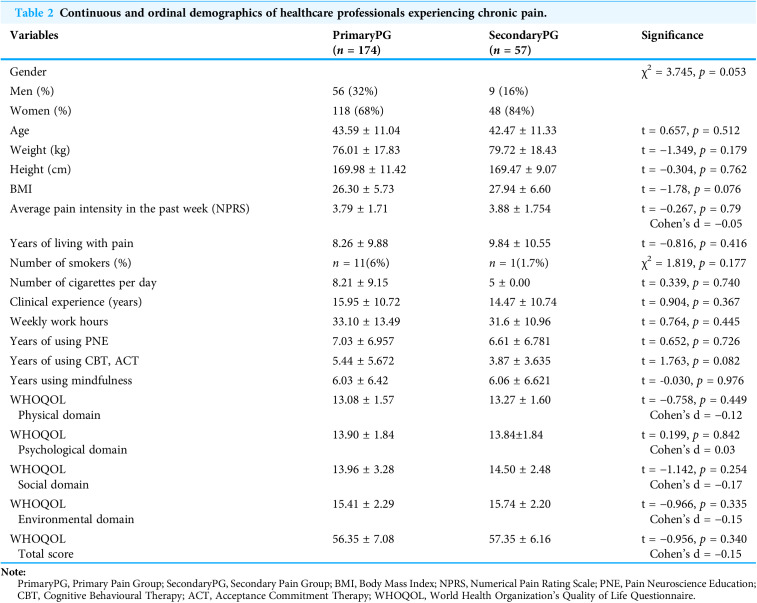
Results: Pain intensity did not significantly differ between primary pain group (4.24 ± 2.21) and secondary pain group (4.37 ± 2.33) (t = -0.267, p = 0.79, Cohen's d = -0.05). The total WHOQOL score was lower in HCPs+CP (66.81 ± 15.74) compared to healthy HCPs (71.13 ± 14.02) (t = -2.136, p = 0.035), but after removing respondents unfamiliar with interventions, no significant differences remained between groups across all WHOQOL domains (-0.09 < Cohen's d < 0.14, p > 0.05). Among the 146 H-HCPs who had recovered from chronic pain, only 11% attributed their recovery to cognitive-based interventions, while the majority credited physical therapy (37.7%) and spontaneous recovery (32.9%).
Conclusion: Despite their specialized knowledge and experience with cognitive-based interventions, HCPs+CP did not report reduced pain intensity, though they maintained quality of life comparable to healthy colleagues. These findings challenge current theoretical models underlying cognitive-based pain management.
期刊介绍:
PeerJ is an open access peer-reviewed scientific journal covering research in the biological and medical sciences. At PeerJ, authors take out a lifetime publication plan (for as little as $99) which allows them to publish articles in the journal for free, forever. PeerJ has 5 Nobel Prize Winners on the Board; they have won several industry and media awards; and they are widely recognized as being one of the most interesting recent developments in academic publishing.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


